A Case of Noncompaction of the Ventricular Myocardium Combined with Situs Ambiguous with Polysplenia
- Affiliations
-
- 1Division of Cardiology Yongdong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. sejoong@yuhs.ac
- 2Division of Radiology, Yongdong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1786225
- DOI: http://doi.org/10.3349/ymj.2007.48.6.1052
Abstract
- A 33-year-old man was admitted to our hospital with chest pain and exertional dyspnea. Two-dimensional echocardiography showed prominent trabeculations and deep intertrabecular recesses, findings consistent with noncompaction of the ventricular myocardium. Thoracoabdominal CT and cardiac magnetic resonance imaging (CMR) revealed situs ambiguous with polysplenia and noncompaction of the left ventricular myocardium. CMR also demonstrated delayed enhancement of the trabeculations located at the apical portion of the left ventricle. The coronary angiogram was normal. This is the first case of noncompaction of the ventricular myocardium associated with situs ambiguous with polysplenia.
MeSH Terms
Figure
-

Fig. 1 Echocardiography revealing prominent trabeculations and deep intertrabecular recesses. The noncompacted areas mainly involve the anterior and inferolateral left ventricular segments.
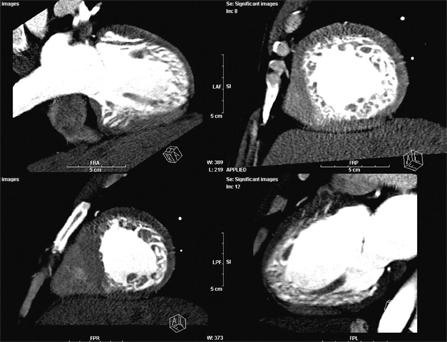
Fig. 2 Chest CT showing the two-layered structure of a thin, compacted epicardial layer and an extremely thick endocardial layer with prominent trabeculations and deep recesses.
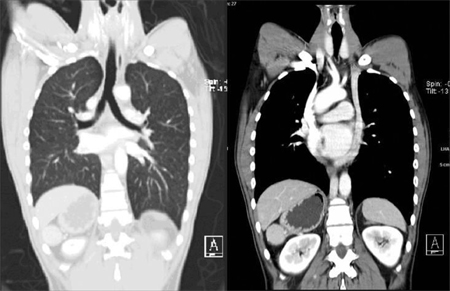
Fig. 3 Chest CT showing bilateral, bilobed lungs, where the main bronchi is seen below the pulmonary artery. Minor fissures are absent, and double superior vena cava and left superior vena cava connect to the coronary sinus.
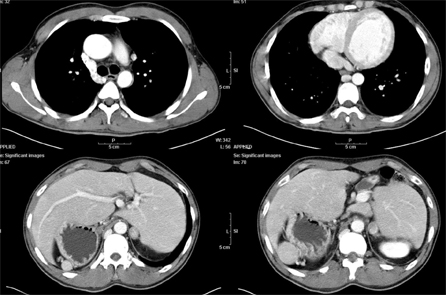
Fig. 4 Abdominal CT showing right-sided stomach and multiple spleens in the right abdomen, persistent accessory azygous drainage to the intrahepatic vein and IVC segment, and interruption of the inferior vena cava.
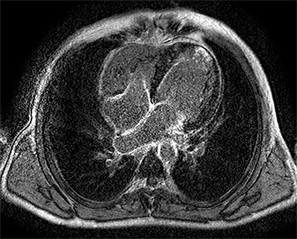
Fig. 5 Delayed enhancement CMR showing the two-layered structure of NVM and hyperenhancement of the trabeculations located at the apical portion of the left ventricle, suggesting areas of fibrosis.
Reference
-
1. Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O'Connell J, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of cardiomyopathies. Circulation. 1996. 93:841–842.2. Sedmera D, Pexieder T, Vuillemin M, Thompson RP, Anderson RH. Developmental patterning of the myocardium. Anat Rec. 2000. 258:319–337.3. Oechslin EN, Attenhofer Jost CH, Rojas JR, Kaufmann PA, Jenni R. Long-term follow-up of 34 adults with isolated left ventricular noncompaction: a distinct cardiomyopathy with poor prognosis. J Am Coll Cardiol. 2000. 36:493–500.4. Moon JY, Chung N, Seo HS, Choi EY, Ha JW, Rim SJ. Noncompaction of the ventricular myocardium combined with polycystic kidney disease. Heart Vessels. 2006. 21:195–198.5. Bellet S, Gouley BA. Congenital heart disease with multiple cardiac anomalies: report of a case showing aortic atresia, fibrous scar in myocardium and embryonal sinusoidal remains. Am J Med Sci. 1932. 183:458–465.6. Chin TK, Perloff JK, Williams RG, Jue K, Mohrmann R. Isolated noncompaction of left ventricular myocardium. A study of eight cases. Circulation. 1990. 82:507–513.7. Jenni R, Oechslin E, Schneider J, Attenhofer Jost C, Kaufmann PA. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: a step towards classification as a distinct cardiomyopathy. Heart. 2001. 86:666–671.8. Ichida F, Tsubata S, Bowles KR, Haneda N, Uese K, Miyawaki T, et al. Novel gene mutations in patients with left ventricular noncompaction or Barth syndrome. Circulation. 2001. 103:1256–1263.9. Dusek J, Oštádal B, Duskova M. Postnatal persistence of spongy myocardium with embryonic blood supply. Arch Pathol. 1975. 99:312–317.10. Feldt RH, Rahimtoola SH, Davis GD, Swan HJ, Titus JL. Anomalous ventricular myocardial patterns in a child with complex congenital heart disease. Am J Cardiol. 1969. 23:732–734.11. Stölberger C, Finsterer J. Left ventricular hypertrabeculation/noncompaction. J Am Soc Echocardiogr. 2004. 17:91–100.12. Peoples WM, Moller JH, Edwards JE. Polysplenia: a review of 146 cases. Pediatr Cardiol. 1983. 4:129–137.13. Tonkin IL. Friedman WF, Higgins CB, editors. The definition of cardiac malpositions with echocardiography and computed tomography. Pediatric cardiac imaging. 1984. Philadelphia, PA: Saunders;157–187.14. Moon JC, Mundy HR, Lee PJ, Mohiaddin RH, Pennell DJ. Images in cardiovascular medicine. Myocardial fibrosis in glycogen storage disease type III. Circulation. 2003. 107:e47.15. Korcyk D, Edwards CC, Armstrong G, Christiansen JP, Howitt L, Sinclair T, et al. Contrast-enhanced cardiac magnetic resonance in a patient with familial isolated ventricular non-compaction. J Cardiovasc Magn Reson. 2004. 6:569–576.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Situs Ambiguous with Polysplenia of Macrosomia
- A case of isolated noncompaction of the ventricular myocardium in an elderly patient
- Noncompaction of Ventricular Myocardium Involving the Right Ventricle
- Incidentally Detected Situs Ambiguous in Adults
- A case of spongy myocardium initially manifested by ventricular tachycardia in adult
