Catheter Ablation of a Left Free-Wall Accessory Pathway via the Radial Artery Approach
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Pusan National University College of Medicine, Busan, Korea. mdjunkim@yahoo.co.kr
- KMID: 1786224
- DOI: http://doi.org/10.3349/ymj.2007.48.6.1048
Abstract
- Catheter ablation of the left free-wall accessory pathways (APs) is normally performed by the retrograde transaortic approach via a femoral artery or the transseptal approach. Here we report a case of an overt left free-wall AP, which was successfully ablated with a retrograde transaortic approach via the radial artery without any vascular complications. The patient has remained free of any symptoms or pre-excitation observed on the ECG during a 10-month post- ablation follow-up.
Keyword
MeSH Terms
Figure
-

Fig. 1 12-lead ECGs during sinus rhythm (A), rapid atrial pacing (B), and an induced supraventricular tachycardia (C).

Fig. 2 Surface lead electrocardiograms and intracardiac electrograms during the baseline (A), ventricular pacing at a cycle length of 320 ms (B) and a supraventricular tachycardia (C). ECG leads I, aVF, and V1 are displayed together with the electrograms from the high right atrium (HRA), proximal to distal His bundle (His), proximal to distal coronary sinus (CS), and right ventricular apex (RVA) catheters.
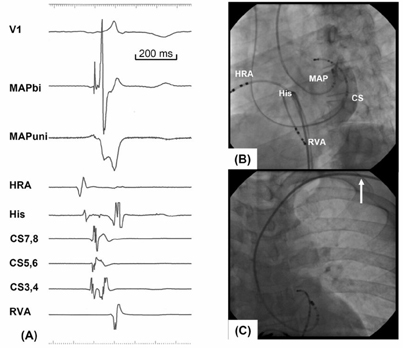
Fig. 3 Intracardiac electrograms (A) and 40° left anterior oblique fluoroscopic view from the ablation site (B). (A) The local electrogram recorded from the mapping catheter (MAP) exhibited a tri-phasic fused atrio-ventricular electrogram with a possible accessory pathway potential, and the unipolar electrogram recorded from the MAP (MAPuni) revealed a QS pattern. (B), (C) The ablation catheter was passed over the left subclavian artery (arrow) and positioned on the mitral annulus.
Reference
-
1. Lesh MD, Van Hare GF, Scheinman MM, Ports TA, Epstein LA. Comparison of the retrograde and transseptal methods for ablation of left free wall accessory pathways. J Am Coll Cardiol. 1993. 22:542–549.2. Park EH, Kim MH, Park TH, Ahn SJ, Jung DS, Paik JH, et al. Feasibility of transradial coronary angiography using a single Judkins left catheter. Korean Circ J. 2005. 35:253–257.3. Slagboom T, Kiemeneij F, Laarman GJ, van der Wieken R. Outpatient coronary angioplasty: feasible and safe. Catheter Cardiovasc Interv. 2005. 64:421–427.4. Han KR, Park WJ, Oh DJ, Park DG, Jung WC, Jung KJ, et al. Feasibility and problems in transradial coronary angiography and intervention. Korean Circ J. 2000. 30:1083–1091.5. Kim JY, Yoon J, Jung HS, Ko JY, Yoo BS, Hwang SO, et al. Feasibility of the radial artery as a vascular access route in performing primary percutaneous coronary intervention. Yonsei Med J. 2005. 46:503–510.6. Choussat R, Black A, Bossi I, Fajadet J, Marco J. Vascular complications and clinical outcome after coronary angioplasty with platelet IIb/IIIa receptor blockade. Comparison of transradial vs transfemoral arterial access. Eur Heart J. 2000. 21:662–667.7. Liu TJ, Lai HC, Lee WL, Wang KY, Wu TJ, Huang JL, et al. Immediate and late outcomes of patients undergoing transseptal left-sided heart catheterization for symptomatic valvular and arrhythmic diseases. Am Heart J. 2006. 151:235–241.8. Swartz JF, Tracy CM, Fletcher RD. Radiofrequency endocardial catheter ablation of accessory atrioventricular pathway atrial insertion sites. Circulation. 1993. 87:487–499.9. Roelke M, Smith AJ, Palacios IF. The technique and safety of transseptal left catheterization: the Massachusetts General Hospital experience with 1,279 procedures. Cathet Cardiovasc Diagn. 1994. 32:332–339.10. Lesh MD, Van Hare GF, Schamp DJ, Chien W, Lee MA, Griffin JC, et al. Curative percutaneous catheter ablation using radiofrequency energy for accessory pathways in all locations: results in 100 consecutive patients. J Am Coll Cardiol. 1992. 19:1303–1309.11. Calkins H, Langberg J, Sousa J, el-Atassi R, Leon A, Kou W, et al. Radiofrequency catheter ablation of accessory atrioventricular connections in 250 pateints. Abbreviated therapeutic approach to Wolff-Parkinson-White syndrome. Circulation. 1992. 85:1337–1346.12. Louvard Y, Benamer H, Garot P, Hildick-Smith D, Loubeyre C, Rigattieri S, et al. Comparison of transradial and transfemoral approaches for coronary angiography and angioplasty in octogenarians (the OCTOPLUS study). Am J Cardiol. 2004. 94:1177–1180.13. Juergens CP, Hallani H, Leung DY, Crozier JA, Robinson JT, Lo S, et al. Comparison of 6 and 7 French guiding catheters for percutaneous coronary intervention: results of a randomised trial with a vascular ultrasound endpoint. Catheter Cardiovasc Interv. 2005. 66:528–534.14. Nikolsky E, Mehran R, Halkin A, Aymong ED, Mintz GS, Lasic Z, et al. Vascular complications associated with arteriotomy closure devices in patients undergoing percutaneous coronary procedure: a meta-analysis. J Am Coll Cardiol. 2004. 44:1200–1209.15. Kim SH, Kim EJ, Kim MK, Yun IS, Park WJ, Han SJ, et al. Comparison of the effects of nicorandil and cocktail solution to prevent radial artery spasm during coronary angiography. Korean Circ J. 2006. 36:133–139.16. Yoo BS, Lee SH, Ko JY, Lee BK, Kim SN, Lee MO, et al. Procedural outcomes of repeated transradial coronary procedure. Catheter Cardiovasc Interv. 2003. 58:301–304.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Left atrial ıntramural hematoma after radiofrequency catheter ablation of left lateral accessory pathway
- Successful Ablation of Resistant Left Lateral Accessory Pathway and Coexisting Atypical Atrioventricular Nodal Reentrant Tachycardia
- Electrophysiologic characteristics of multiple accessory pathways
- Ablation of manifest left free wall accessory pathways with polarity reversal mapping: ventricular approach
- Characteristics of Intracardiac Electrogram at Successful Sites of Radiofrequency Catheter Ablation in Patients with Accessory Pathways
