Successful Ablation of Resistant Left Lateral Accessory Pathway and Coexisting Atypical Atrioventricular Nodal Reentrant Tachycardia
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Inje University College of Medicine, Ilsan Paik Hospital, Goyang, Korea. jnamgung@paik.ac.kr
- KMID: 2224964
- DOI: http://doi.org/10.4070/kcj.2013.43.3.189
Abstract
- A 41-year-old male was presented with drug-resistant supraventricular tachycardia. Electrophysiological study confirmed that the supraventricular tachycardia was caused by dual atrioventricular nodal pathways and a left lateral accessory pathway (AP). The left lateral AP was resistant to traditional endocardial ablation, but was successfully eliminated by radiofrequency ablation via the intracoronary sinus approach.
Keyword
MeSH Terms
Figure
-

Fig. 1 Simultaneous recordings for surface leads I, aVF, V1 and intracardiac electrograms from high right atrium, proximal and distal coronary sinus, His bundle, and right ventricular apex. Earliest atrial (A) activation during right ventricular (V) pacing (A) or spontaneous supraventricular tachycardia induction are recorded from the CS1, 2 electrodes (B). The atrial activation sequence is eccentric and earliest at the distal coronary sinus. HIS: His bundle, RVA: right ventricular apex, HRA: high right atrium, CS: coronary sinus, ABL: ablation.

Fig. 2 Ablation of resistant left lateral accessory pathway via the intracoronary sinus approach. A and B: the fluoroscopic images, right anterior oblique and left anterior oblique, showing the position of ablation catheter at distal coronary sinus through intracoronary sinus. C: the local electrogram from distal ABL catheter during right ventricle (RV) pacing has the same ventricular (V) and atrial (A) timing compared to that of proximal CS catheter. D: after radiofrequency energy (RF) application at this point, the electrogram shows the retrograde conduction through HIS during RV pacing. HIS: His bundle, RVA: right ventricular apex, HRA: high right atrium, CS: coronary sinus, ABL: ablation.

Fig. 3 Initiation of atypical atrioventricular nodal reentrant tachycardia (AVNRT) with programmed atrial stimulation (550/280 msec); AH jump and the induction of atypical AVNRT with antegrade conduction (downward arrow) by fast pathway and retrograde conduction (upward arrow) by slow pathway. The tachycardia cycle length is 342 msec, AH interval is 140 msec, HA interval is 210 msec, AH/HA ratio <1 and VA interval is 185 msec. HRA: high right atrium, HIS: His bundle, ABL: ablation, CS: coronary sinus, RV: right ventricular.
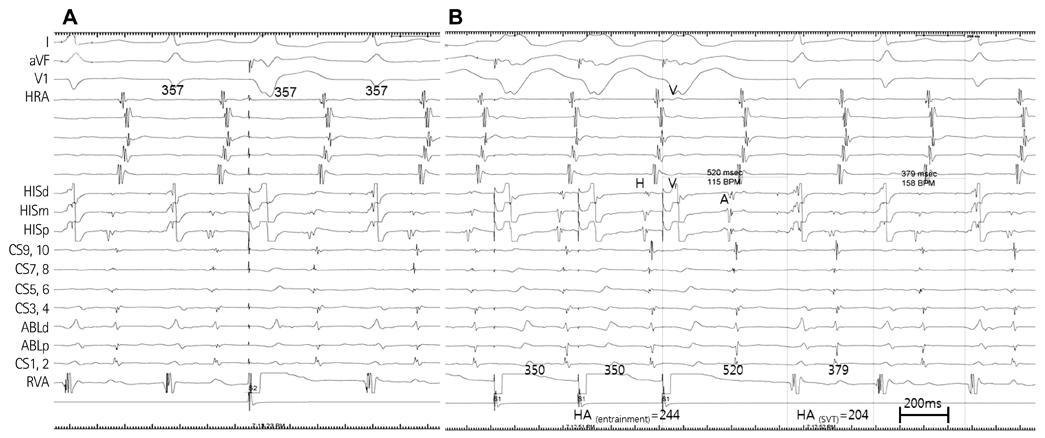
Fig. 4 Ablation of atypical atrioventricular nodal reentrant tachycardia. A: delivery of a ventricular premature depolarization when the HIS is refractory cannot advance the atrial activation. B: during atypical atrioventricular nodal reentrant tachycardia, following cessation of ventricular entrainment pacing, the tachycardia resumes with a V-A-V response. The values of post-pacing interval (PPI) minus tachycardia cycle length (TCL) were greater than 115 msec and the ΔHA=40 msec. HRA: high right atrium, HIS: His bundle, CS: coronary sinus, ABL: ablation, RVA: right ventricular apex.
Reference
-
1. Chen YJ, Chen SA, Chiang CE, et al. Dual AV node pathway physiology in patients with Wolff-Parkinson-White syndrome. Int J Cardiol. 1996. 56:275–281.2. Becker AE, Anderson RH, Durrer D, Wellens HJ. The anatomical substrates of wolff-parkinson-white syndrome. A clinicopathologic correlation in seven patients. Circulation. 1978. 57:870–879.3. Jackman WM, Wang XZ, Friday KJ, et al. Catheter ablation of accessory atrioventricular pathways (Wolff-Parkinson-White syndrome) by radiofrequency current. N Engl J Med. 1991. 324:1605–1611.4. Calkins H, Langberg J, Sousa J, et al. Radiofrequency catheter ablation of accessory atrioventricular connections in 250 patients. Abbreviated therapeutic approach to Wolff-Parkinson-White syndrome. Circulation. 1992. 85:1337–1346.5. Lesh MD, Van Hare GF, Schamp DJ, et al. Curative percutaneous catheter ablation using radiofrequency energy for accessory pathways in all locations: results in 100 consecutive patients. J Am Coll Cardiol. 1992. 19:1303–1309.6. Haissaguerre M, Gaita F, Fischer B, Egloff P, Lemetayer P, Warin JF. Radiofrequency catheter ablation of left lateral accessory pathways via the coronary sinus. Circulation. 1992. 86:1464–1468.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of AV reentrant tachycardia utilizing a left lateral accessory pathway with long VA conduction time
- Atrioventricular Nodal Reentrant Tachycardia (AVNRT)
- Radiofrequency Catheter Ablation of Atrioventricular Nodal Reentrant Tachycardia in Two Patients with Persistent Left Superior Vena Cava
- Clinical Experiences in Radiofrequency Catheter Ablation
- Familial Occurrence of Atrioventricular Nodal Reentrant Tachycardia in a Mother and Her Son
