Multislice CT Virtual Intravascular Endoscopy for Assessing Pulmonary Embolisms: a Pictorial Review
- Affiliations
-
- 1Discipline of Medical Imaging, Department of Imaging and Applied Physics, Curtin University of Technology, Perth, Western Australia, Australia. z.sun@curtin.edu.au
- 2Department of Radiology, Kind Saud Hospital, Riyadh, Saudi Arabia.
- 3Department of Radiology, Military Hospital, Riyadh, Saudi Arabia.
- KMID: 1783199
- DOI: http://doi.org/10.3348/kjr.2010.11.2.222
Abstract
- Multislice CT has been widely used in clinical practice for diagnosing cardiovascular disease due to its reduced invasiveness and its high spatial and temporal resolution. As a reliable alternative to conventional pulmonary angiography, multislice CT angiography has been recognized as the first line technique for detecting and diagnosing pulmonary embolism. A pulmonary embolism located in the main pulmonary artery, as well as being located in the segmental branches, can be accurately detected with multislice CT imaging, and especially with the use of 16- and 64-slice CT scanners. Visualization of pulmonary embolisms has traditionally been limited to 2D, multiplanar reformation and the 3D external surface visualizations. In this pictorial review, we present our experience of using 3D virtual intravascular endoscopy to characterize and evaluate the intraluminal appearance of pulmonary embolisms in a group of patients who were suspected of having pulmonary embolism and who were undergoing multislice CT angiography. We expect that the research findings from this study will provide insight into the extent of disease and the luminal changes to the pulmonary arteries that are due to the presence of thrombus, and so monitoring of the progress of disease and predicting the treatment outcome can well be achieved.
MeSH Terms
-
Adolescent
Adult
Aged
Aged, 80 and over
Contrast Media/diagnostic use
Endoscopy/*methods
Female
Humans
Imaging, Three-Dimensional/methods
Iohexol/diagnostic use
Male
Middle Aged
Pulmonary Artery/radiography
Pulmonary Embolism/*radiography
Radiographic Image Enhancement/methods
Radiographic Image Interpretation, Computer-Assisted/*methods
Tomography, X-Ray Computed/*methods
User-Computer Interface
Young Adult
Figure
-
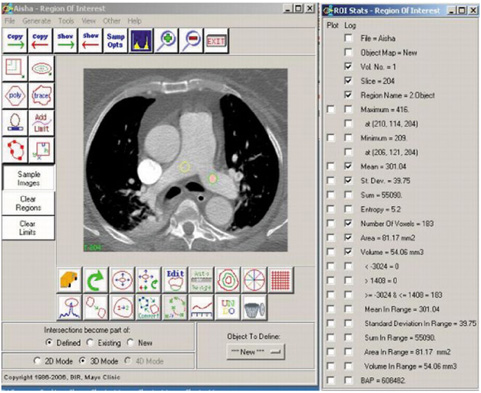
Fig. 1 Measurement of signal to noise ratio. Circular region of interest with minimum area of 50 mm2 is placed at bilateral main pulmonary arteries to measure mean CT attenuation and image noise, and latter is described as standard deviation. Signal to noise ratio is calculated by dividing CT attenuation by standard deviation.

Fig. 2 Normal main pulmonary arteries visualized on virtual intravascular endoscopy. Measured signal to noise ratios were 19 and 24 at right and left pulmonary arteries, respectively. LPA = left pulmonary artery, RPA = right pulmonary artery

Fig. 3 Virtual intravascular endoscopy visualization of pulmonary embolism in right pulmonary artery is affected by high density contrast in superior vena cava. Measured signal to noise ratio was 8.9 at right pulmonary artery. Beam-hardening streak artifact (arrows in A) causes irregular appearance of right pulmonary artery visualized on virtual intravascular endoscopy (B). Corresponding orthogonal views confirm that irregular luminal change (C) is caused by artifact. Arrows in B and C indicate irregular wall changes that are due to artifact. RLA = right lower lobar artery, RUA = right upper lobar artery.

Fig. 4 Virtual intravascular endoscopy visualization of pulmonary embolism in right main pulmonary artery. CT attenuation of thrombus is measured to be 35.87 HU (A), and it appears as protruding sign (arrows in B) inside pulmonary artery after applying upper CT threshold of 250 HU to remove contrast-enhanced blood. Arrowhead refers to artifacts caused by high density in superior vena cava.

Fig. 5 Pulmonary embolism involving bilateral pulmonary artery branches. Large thrombus is present in left main pulmonary artery and it extends to right side (A). Orthogonal views show that viewing position is located in pulmonary trunk (B). C and D demonstrate continuous extension of thrombus from proximal part of main pulmonary artery to distal segment with lumen narrowing, as well as protruding sign in lumen.
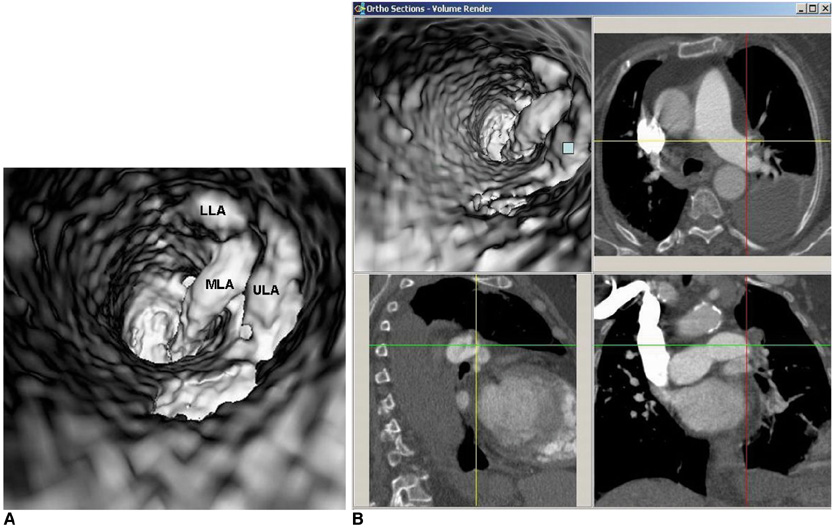
Fig. 6 Virtual intravascular endoscopy visualization of multiple emboli in left lobar arteries (A). Multiplanar views help to confirm that location of thrombus corresponds to involved lobar artery (B). Blue box indicates viewing position placed at left upper lobar thrombus. LLA = lower lobar artery, MLA = middle (lingular) lobar artery, ULA = upper lobar artery

Fig. 7 Virtual intravascular endoscopy views of left lower lobar embolism from proximal to distal segments of lobar artery (A, B). Accurate position of thrombus is confirmed with using multiplanar views (C).
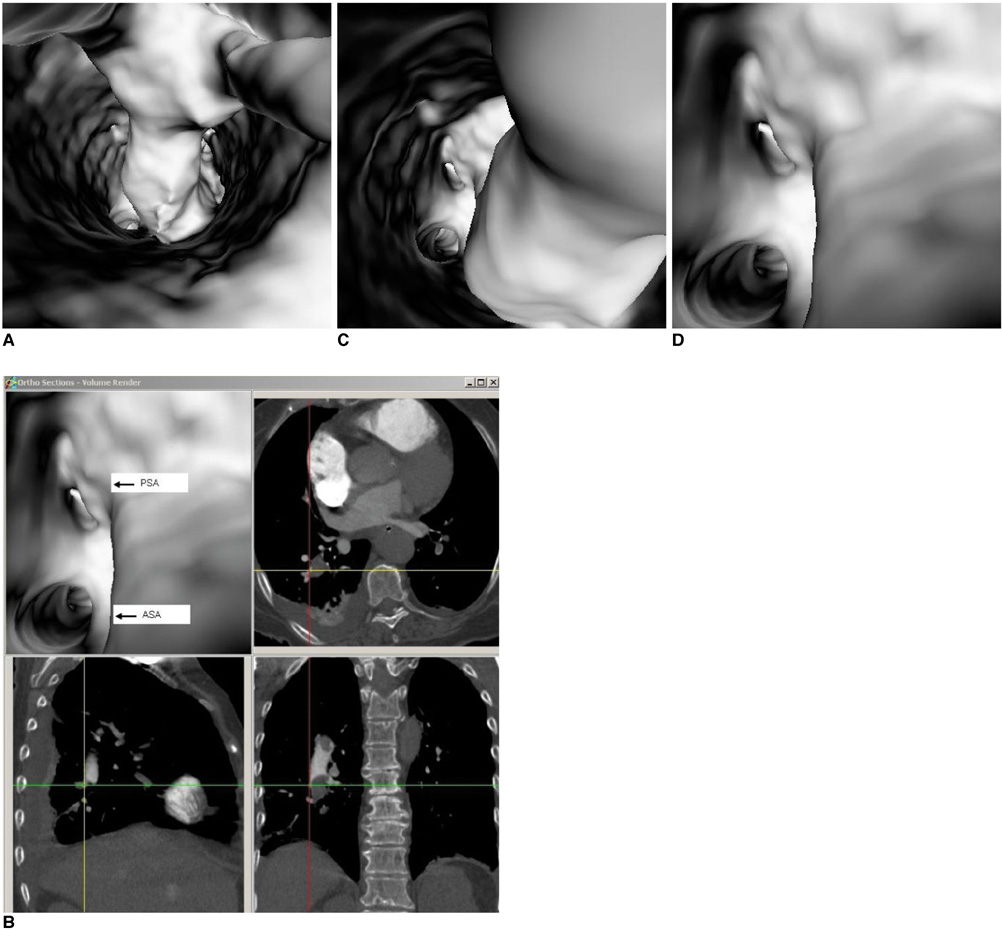
Fig. 8 Virtual intravascular endoscopy views of right posterobasal segmental embolism. Thrombus extends from right lower lobar artery (A) to posterobasal segmental arteries (B, C). Corresponding orthogonal view confirms that position of thrombus is located in right posterobasal segmental artery with compressing corresponding posterobasal segmental artery (D). ASA = anteromedial basal segmental artery, PSA = posterobasal segmental artery
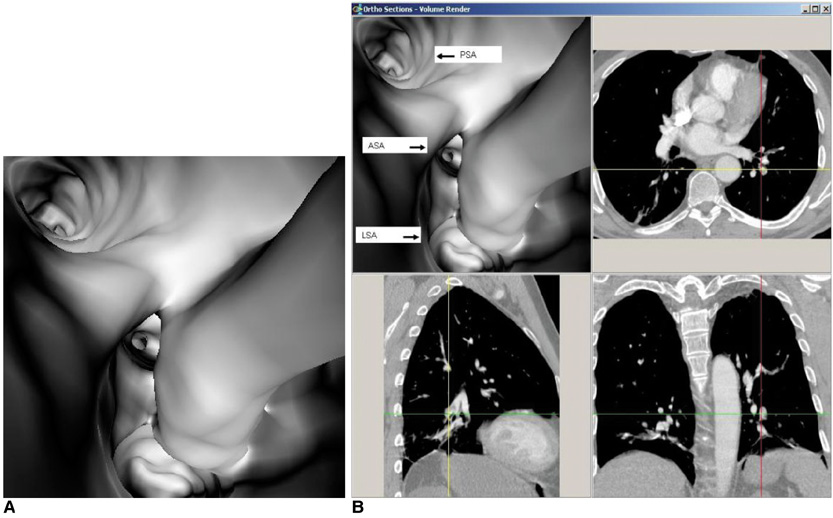
Fig. 9 Virtual intravascular endoscopy views of left lower pulmonary segmental embolism involving two arterial branches. Left lateral basal and anteromedial basal segmental arteries become narrowed due to presence of thrombus (A), while left posterobasal segmental artery is normal. Corresponding orthogonal views (B) confirm relationship between thrombus and segmental artery branches. ASA = anteromedial basal segmental artery, LSA = lateral basal segmental artery, PSA = posterobasal segmental artery
Reference
-
1. Stein PD, Athanasoulis C, Alavi A, Greenspan RH, Hales CA, Saltzman HA, et al. Complications and validity of pulmonary angiography in acute pulmonary embolism. Circulation. 1992. 85:462–468.2. Mills SR, Jackson DC, Older RA, Heaston DK, Moore AV. The incidence, etiologies, and avoidance of complications of pulmonary angiography in a large series. Radiology. 1980. 136:295–299.3. Diffin DC, Leyendecker JR, Johnson SP, Zucker RJ, Grebe PJ. Effect of anatomic distribution of pulmonary emboli on interobserver agreement in the interpretation of pulmonary angiography. AJR Am J Roentgenol. 1998. 171:1085–1089.4. Meaney JF, Weg JG, Chenevert TL, Stafford-Johnson D, Hamilton BH, Prince MR. Diagnosis of pulmonary embolism with magnetic resonance angiography. N Engl J Med. 1997. 336:1422–1427.5. Oudkerk M, van Beek EJ, Wielopolski P, van Ooijen PM, Brouwers-Kuyper EM, Bongaerts AH, et al. Comparison of contrast-enhanced magnetic resonance angiography and conventional pulmonary angiography for the diagnosis of pulmonary embolism: a prospective study. Lancet. 2002. 359:1643–1647.6. Keilholz SD, Bozlar U, Fujiwara N, Mata JF, Berr SS, Corot C, et al. MR diagnosis of a pulmonary embolism: comparison of P792 and Gd-DOTA for first pass perfusion MRI and contrast-enhanced 3D MRA in a rabbit model. Korean J Radiol. 2009. 10:447–454.7. British Thoracic Society Standards of Care Committee Pulmonary Embolism Guideline Development Group. British Thoracic Society guidelines for the management of suspected acute pulmonary embolism. Thorax. 2003. 58:470–483.8. Hayashino Y, Goto M, Noguchi Y, Fukui T. Ventilation-perfusion scanning and helical CT in suspected pulmonary embolism: meta-analysis of diagnostic performance. Radiology. 2005. 234:740–748.9. Guilabert JP, Manzur DN, Tarrasa MJ, Llorens ML, Braun P, Arques MP. Can multislice CT alone run out reliably pulmonary embolism? A prospective study. Eur J Radiol. 2007. 62:220–226.10. Schoepf UJ, Goldhaber SZ, Costello P. Spiral computed tomography for acute pulmonary embolism. Circulation. 2004. 109:2160–2167.11. Rathbun SW, Raskob GE, Whitsett TL. Sensitivity and specificity of helical computed tomography in the diagnosis of pulmonary embolism: a systematic review. Ann Intern Med. 2000. 132:227–232.12. Van Strijen MJ, De Monye W, Kieft GJ, Pattynama PM, Prins MH, Huisman MV. Accuracy of single-detector spiral CT in the diagnosis of pulmonary embolism: a prospective multicenter cohort study of consecutive patients with abnormal perfusion scintigraphy. J Thromb Haemost. 2005. 3:17–25.13. Perrier A, Roy PM, Sanchez O, Le Gal G, Meyer G, Gourdier AL, et al. Multidetector-row computed tomography in suspected pulmonary embolism. N Engl J Med. 2005. 352:1760–1768.14. Sun Z, Winder RJ, Kelly BE, Ellis PK, Hirst DG. CT virtual intravascular endoscopy of abdominal aortic aneurysms treated with suprarenal endovascular stent grafting. Abdom Imaging. 2003. 28:580–587.15. Sun Z, Winder RJ, Kelly BE, Ellis PK, Kennedy PT, Hirst DG. Diagnostic value of CT virtual intravascular endoscopy in aortic stent-grafting. J Endovasc Ther. 2004. 11:13–25.16. Sun Z, Allen YB, Nadkarni S, Knight R, Hartley DE, Lawrence-Brown MM. CT virtual intravascular endoscopy in the visualization of fenestrated stent-grafts. J Endovasc Ther. 2008. 15:42–51.17. Sun Z. 3D multislice CT angiography in post-aortic stent grafting: a pictorial essay. Korean J Radiol. 2006. 7:205–211.18. Sun Z, Mwipatayi BP, Allen YB, Hartley DE, Lawrence-Brown MM. Multislice CT angiography of fenestrated endovascular stent grafting for treating abdominal aortic aneurysms: a pictorial review of the 2D/3D visualizations. Korean J Radiol. 2009. 10:285–293.19. Wittram C, Maher MM, Yoo AJ, Kalra MK, Shepard JA, McLoud TC. CT angiography of pulmonary embolism: diagnostic criteria and causes of misdiagnosis. Radiographics. 2004. 24:1219–1238.20. Jones SE, Wittram C. The indeterminate CT pulmonary angiogram: imaging characteristics and patient clinical outcome. Radiology. 2005. 237:329–337.21. Yavas US, Calisir C, Ozkan IR. The interobserver agreement between residents and experienced radiologists for detecting pulmonary embolism and DVT with using CT pulmonary angiography and indirect CT venography. Korean J Radiol. 2008. 9:498–502.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 3D Multislice CT Angiography in Post-Aortic Stent Grafting: A Pictorial Essay
- Pulmonary and Renal Cement Embolisms During Balloon Kyphoplasty: A Case Report
- Virtual Endoscopy of Impacted Foreign Bodies in Tracheal and Esophageal Model
- Virtual CT Colonoscopy and Virtual CT Barium Enema using Multidetector-row CT
- Virtual Endoscopy Using Spiral CT in Head and Neck Lesions
