3D Multislice CT Angiography in Post-Aortic Stent Grafting: A Pictorial Essay
- Affiliations
-
- 1Discipline of Medical Imaging, Department of Imaging and Applied Physics, Curtin University of Technology, Perth, Western Australia. z.sun@curtin.edu.au
- KMID: 1114354
- DOI: http://doi.org/10.3348/kjr.2006.7.3.205
Abstract
- Helical CT angiography has been widely used in both pre- and post-aortic stent grafting and it has been confirmed to be the preferred modality when compared to conventional angiography. The recent development of multislice CT (MSCT) has further enhanced the applications of CT angiography for aortic stent grafting. One of the advantages of MSCT angiography over conventional angiography is that the 3D reconstructions, based on the volumetric CT data, provide additional information during follow-up of aortic stent grafting. While endovascular repair has been increasingly used in clinical practice, the use of 3D MSCT imaging in endovascular repair continues to play an important role. In this pictorial essay, we aimed to discuss the diagnostic performance of 3D MSCT angiography in post aortic stent grafting, including the most commonly used surface shaded display, curvilinear reformation, the maximum intensity projection, volume rendering and virtual endoscopy. The advantages and disadvantages of each 3D reconstruction are also explored.
MeSH Terms
Figure
-
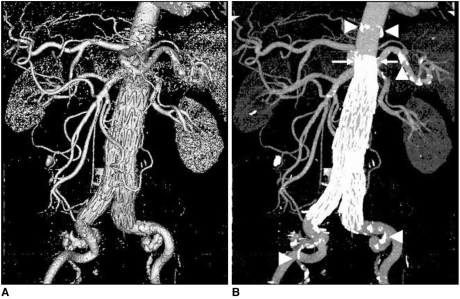
Fig. 1 An 84-year-old man with an infrarenal abdominal aortic aneurysm was treated with an aortic stent graft and he was followed-up at 48 months. The multislice CT surface shaded display clearly shows the aortic branches and the stent graft. The corresponding multislice CT maximum-intensity projection image clearly demonstrates the calcification in the aortic wall besides the aortic stent graft, and the arterial branches. The suprarenal stent grafts are shown deployed above the renal arteries (arrows). Arrowheads point to the calcification. (Reprint with permission from Ref 13)

Fig. 2 A. Surface shaded display image in an 80-year-old man shows abdominal aortic aneurysm after endovascular repair. Although the aortic branches can be visualised, calcifications in the aortic wall cannot be clearly demonstrated when compared to the corresponding maximum-intensity projection image as shown in figure 2B (arrows).
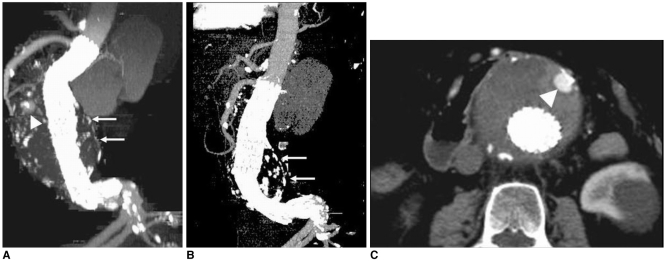
Fig. 3 A 74-year-old man was found to have distal stent migration of 10.2 mm due to foreshortening of the longitudinal aneurysm sac at a 24-month follow-up period (A, B). Arrows in A and B indicate the aneurysm sac, while arrowheads in A and C point to a type II endoleak due to retrograde flow of the patent inferior mesenteric artery, which resolved spontaneously.(Reprint with permission from Ref 13)
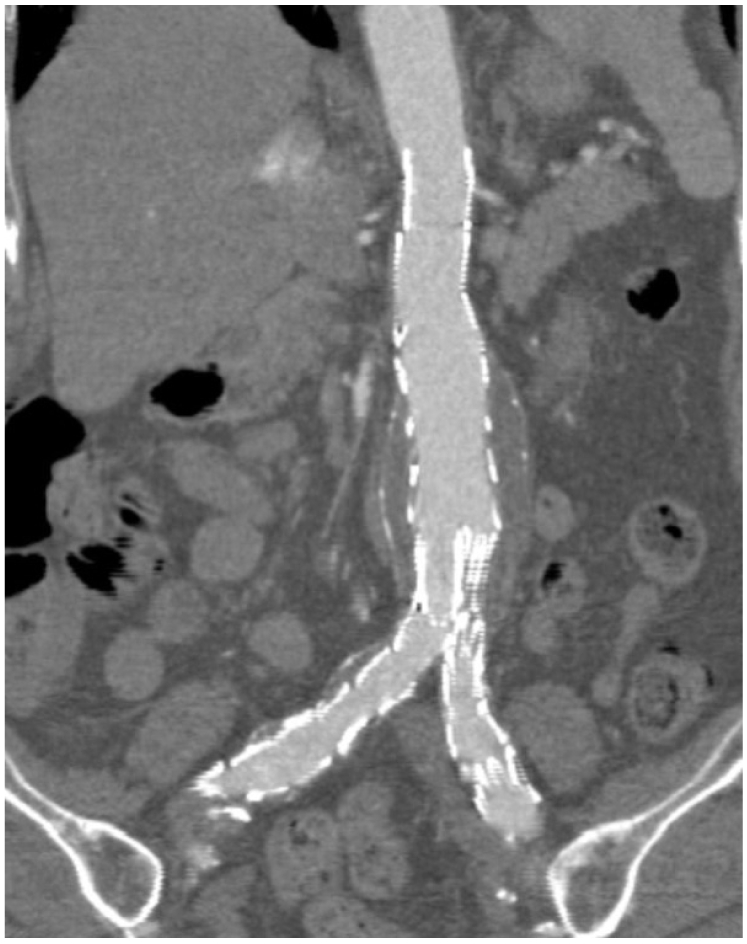
Fig. 4 Curvilinear reformation reconstructions in a patient following endovascular repair of abdominal aortic aneurysm. The aortic branches, the stent graft and the aneurysm sac are shown altogether in the figure.
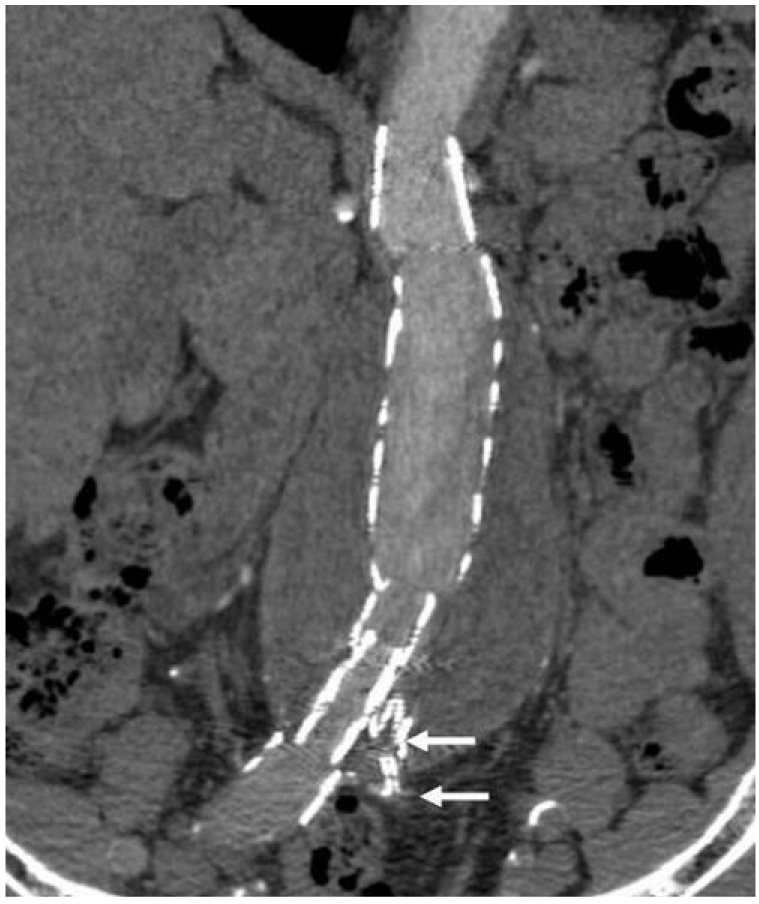
Fig. 5 Curvilinear reformation reconstruction in another patient after endovascular repair of abdominal aortic aneurysm. In contrast to what is shown in figure 4, not all of the information is displayed in this image and the left common iliac artery is missing (arrows) as this anatomy is not in the selected plane.
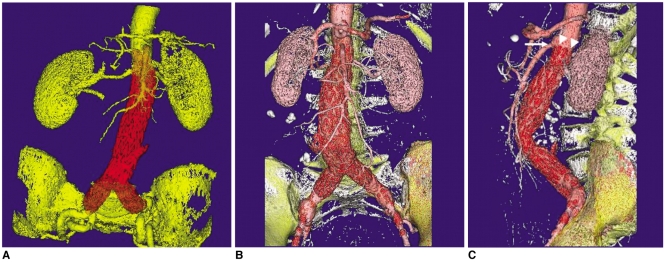
Fig. 6 3D volume rendering images were generated in a 65-year-old woman at 36 months after endovascular repair. Different colours were applied to various structures, including the aortic stent graft, arteries and bones (A-C). As shown in the sagittal view (C), the top of the suprarenal stent (arrowheads) was placed just below the superior mesenteric (arrow) artery.
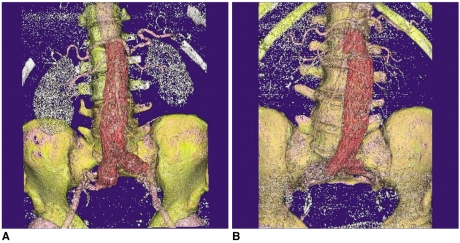
Fig. 7 3D volume rendering images were acquired in two patients with suboptimal source image quality, which affects the visualization of the anatomical structures on volume rendering. The signal to noise ratio measured in these two cases was less than 10 (6-8.2) at the levels of the renal artery and the common iliac arteries, which resulted in poor demonstration of the renal parenchyma or the common iliac arteries (A, B).
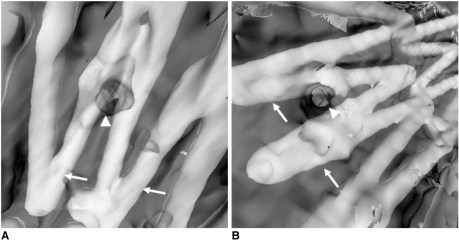
Fig. 8 Virtual intravascular endoscopy images acquired from two patients after endovascular repair of abdominal aortic aneurysms shows the different encroachment of stent wires to the renal ostia. Two stent wires were shown to cross the left renal ostium peripherally in A, while one stent wire crosses the right renal ostium peripherally as shown in B. Arrows indicate the stent wires, while arrowheads point to the renal ostia.
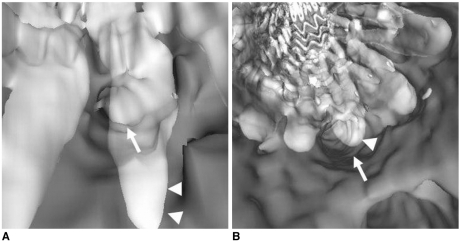
Fig. 9 An 81-year-old woman with an abdominal aortic aneurysm was treated with a suprarenal stent graft and she was followed-up at 36 months. A 10.2 mm stent migration was noted in the most recent CT maximum-intensity projection image (B) when compared to the previous one (A). Virtual intravascular endoscopy shows that the superior mesenteric artery ostium was encroached by stent wire, but its position of encroachment shifted due to the movement of stent wires, which was caused by the longitudinal foreshortening of the aneurysm sac. The superior mesenteric artery ostium seems to be covered more than 50% by the stent wire due to the overestimated thickness of wire diameter. The arrow denotes the superior mesenteric artery, while arrowheads refer to the stent wires. (Reprint with permission from Ref 13)
Cited by 1 articles
-
Value of 3-Dimensional CT Virtual Anatomy Imaging in Complex Foreign Body Retrieval from Soft Tissues
Xiu-Jun Yang, Guang-Fu Xing, Chang-Wen Shi, Wei Li
Korean J Radiol. 2013;14(2):269-277. doi: 10.3348/kjr.2013.14.2.269.
Reference
-
1. Buth J, van Marrewijk CJ, Harris PL, Hop WC, Riambau V, Laheij RJF, et al. Outcome of endovascular abdominal aortic aneurysm repair in patients with conditions considered unfit for an open procedure: a report on the EUROSTAR experience. J Vasc Surg. 2002; 35:211–221. PMID: 11854717.
Article2. Cao P, Verzini F, Parlani G, Romano L, De Rango P, Pagliuca V, et al. Clinical effect of abdominal aortic aneurysm endografting: 7-year concurrent comparison with open repair. J Vasc Surg. 2004; 40:841–848. PMID: 15557895.
Article3. Prinssen M, Verhoeven EL, Buth J, Cuypers PW, van Sambeek MR, Balm R, et al. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004; 351:1607–1618. PMID: 15483279.
Article4. Broeders IA, Blankensteijn JD, Olree M, Mali W, Eikelboom BC. Preoperative sizing of grafts for transfemoral endovascular aneurysm management: a prospective comparative study of spiral CT angiography, arteriography and conventional CT imaging. J Endovasc Surg. 1997; 4:252–261. PMID: 9291050.
Article5. Armerding MD, Rubin GD, Beaulieu CF, Slonim SM, Olcott EW, Samuels SL, et al. Aortic aneurysmal disease: assessment of stent-graft treatment-CT versus conventional angiography. Radiology. 2000; 215:138–146. PMID: 10751479.
Article6. Hu H, He HD, Foley WD, Fox SH. Four multidetector-row helical CT: image quality and volume coverage speed. Radiology. 2000; 215:55–62. PMID: 10751468.
Article7. Rubin GD, Shiau MC, Leung AN, Kee ST, Logan LJ, Sofilos MC. Aorta and iliac arteries: single versus multiple detector-row helical CT angiography. Radiology. 2000; 215:670–676. PMID: 10831682.
Article8. Sun Z, Winder RJ, Kelly BE, Ellis PK, Kennedy PT, Hirst DG. Diagnostic value of CT virtual intravascular endoscopy in aortic stent grafting. J Endovasc Ther. 2004; 11:13–25. PMID: 14748633.9. Sun Z, Winder RJ, Kelly BE, Ellis PK, Hirst DG. CT virtual intravascular endoscopy of abdominal aortic aneurysms treated with suprarenal endovascular stent grafting. Abdom Imaging. 2003; 28:580–587. PMID: 14580104.
Article10. Davis CP, Ladd ME, Romanowski BJ, Wildermuth S, Knoplioch JF, Debatin JF. Human aorta: preliminary results with virtual endoscopy based on three-dimensional MR imaging data sets. Radiology. 1996; 199:37–40. PMID: 8633169.
Article11. Neri E, Bonanomi C, Vignali R, Cioni R, Ferrari M, Petruzzi P, et al. Spiral CT virtual endoscopy of abdominal arteries: clinical applications. Abdom Imaging. 2000; 25:59–61. PMID: 10652924.
Article12. Luccichenti G, Cademartiri F, Pezzella FR, Runza G, Belgrano M, Midiri M, et al. 3D reconstruction techniques made easy: know-how and pictures. Eur Radiol. 2005; 15:2146–2156. PMID: 15809826.
Article13. Sun Z. Three-dimensional visualization of suprarenal aortic stent-grafts: evaluation of migration in midterm follow-up. J Endovasc Ther. 2006; 13:85–93. PMID: 16445328.14. Sun Z, Zheng H. Helical CT angiography of aortic stent grafting: Comparison of three-dimensional rendering techniques. Lecture Notes in Computer Sciences. 2004; 3314:544–549.
Article15. Sun Z, Zheng H. Cross-sectional area reduction of the aortic ostium by suprarenal stent wires: in vitro phantom study by CT virtual angioscopy. Comput Med Imaging Graph. 2004; 28:345–351. PMID: 15294312.
Article16. Willmann JK, Baumert B, Schertler T, Wildermuth S, Pfammatter T, Verdun FR, et al. Aortoiliac and lower extremity arteries assessed with 16-detector row CT angiography: prospective comparison with digital subtraction angiography. Radiology. 2005; 236:1083–1093. PMID: 16055691.
Article17. Schertler T, Wildermuth A, Alkadhi H, Kruppa M, Marincek B, Boehm T. Sixteen-detector row CT angiography for lower-leg arterial occlusive disease: analysis of section width. Radiology. 2005; 237:649–656. PMID: 16244274.
Article18. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005; 46:552–557. PMID: 16053973.
Article19. Flohr T, Stierstorfer K, Raupach R, Ulzheimer S, Bruder H. Performance evaluation of a 64-slice CT system with z-flying focal spot. Rofo. 2004; 176:1803–1810. PMID: 15573292.
Article20. Rydberg J, Kopecky KK, Lalka SG, Johnson MS, Dalsing MC, Persohn SA. Stent grafting of abdominal aortic aneurysms: pre- and postoperative evaluation with multislice helical CT. J Comput Assist Tomogr. 2001; 25:580–586. PMID: 11473190.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multislice CT Angiography of Fenestrated Endovascular Stent Grafting for Treating Abdominal Aortic Aneurysms: a Pictorial Review of the 2D/3D Visualizations
- Multislice CT Virtual Intravascular Endoscopy for Assessing Pulmonary Embolisms: a Pictorial Review
- The Utility of 64 Channel Multidetector CT Angiography for Evaluating the Renal Vascular Anatomy and Possible Variations: a Pictorial Essay
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Fenestrated Stent Graft Repair of Abdominal Aortic Aneurysm: Hemodynamic Analysis of the Effect of Fenestrated Stents on the Renal Arteries
