Preoperative and Postoperative Evaluation of Multiple Giant Coronary Aneurysms by the Use of Coronary CT Angiography with 64-MDCT: A Case of Multiple Giant Coronary Aneurysms Treated with Aneurysmectomy and Coronary Artery Bypass Surgery
- Affiliations
-
- 1Department of Internal Medicine, Vision 21 Cardiac and Vascular Center, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea. hmchoi49@naver.com
- 2Department of Radiology, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
- KMID: 1782984
- DOI: http://doi.org/10.3349/ymj.2009.50.1.160
Abstract
- A coronary artery aneurysm is an uncommon disorder and is seen as a characteristic dilatation of a localized portion of the coronary artery. Clinical manifestation of a coronary artery aneurysm varies from an asymptomatic presentation to sudden death of a patient. Although coronary aneurysms are typically diagnosed by the use of coronary angiography, a new generation of coronary 64-slice multidetector computed tomography (64-MDCT) scanners have successfully been used for evaluating this abnormality in a noninvasive manner. In the present case, we performed coronary 64-MDCT scanning preoperatively and postoperatively on a patient with multiple giant coronary aneurysms. The use of coronary 64-MDCT may provide an evaluation technique not only for diagnosis but also for follow-up after surgery for this condition.
Keyword
MeSH Terms
Figure
-

Fig. 1 Coronary 64-MDCT scan images (A) and an apical two-chamber view of transthoracic echocardiography (B). Three-dimensional images using the volume rendered technique (left) and curved multi-planar reformation (right) show 3 large aneurysms-1 aneurysm from the ramus intermedius (a) and two aneurysms from the circumflex artery (b and c). The largest aneurysm was measured 3.0 × 3.5 cm (black arrows) and had central low attenuation from the liquefied thrombus (mean CT number of 30 Hounsfield units) (c). The second aneurysm of the left circumflex artery is noted next to the largest aneurysm and shows strong homogenous enhancement (b). The distal circumflex artery shows multiple small saccular dilatations (double arrows). Many small collateral vessels and the vascular bed are less clearly enhanced by contrast material due to slow blood flow (white arrows in A). A round, spherical, and echogenic mass (white arrows of 1B) is seen adjacent to the left atrial appendage. LAD, left anterior descending; LM, left main artery; RCA, right coronary artery; LA, left atrium; LV, left ventricle.
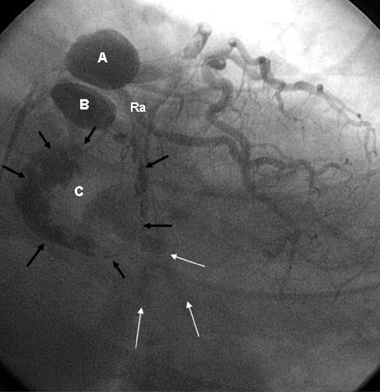
Fig. 2 A conventional coronary angiographic image at a right anterior oblique-caudal view. Two aneurysms are homogenously enhanced by contrast (A and B). The largest aneurysm shows irregular enhancement in the periphery (black arrows), and most of the central area are filled with thrombus (C). The second aneurysm of the left circumflex artery shows homogenous filling with contrast material (B). Faint contrast staining is noted on the distal side of the largest aneurysm (white arrows). A delayed image might have shown collaterals that were seen on CT angiography. Ra, ramus intermedius; CT, computed tomography.
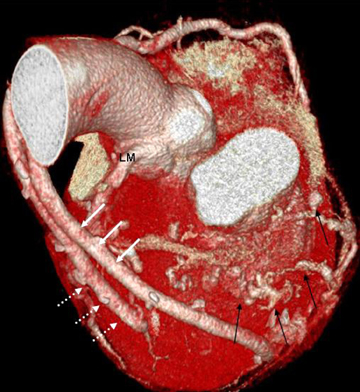
Fig. 3 Coronary 64-MDCT images after surgical repair of the aneurysms and CABG. Three-dimensional images using the volume rendered technique show 2 free venous grafts connecting the distal ramus (white dotted arrows) and distal circumflex artery (white solid arrows). The aneurysms are no longer seen. Collateral vessels and distal circumflex arteries are better defined after the removal of the aneurysms (black arrows). LM, left main; 64-MDCT, 64-slice multidetector computed tomography; CABG, coronary artery bypass graft.
Reference
-
1. Swaye PS, Fisher LD, Litwin P, Vignola PA, Judkins MP, Kemp HG, et al. Aneurysmal coronary artery disease. Circulation. 1983. 67:134–138.
Article2. Ercan E, Tengiz I, Yakut N, Gurbuz A. Large atherosclerotic left main coronary aneurysm: a case report and review of literature. Int J Cardiol. 2003. 88:95–98.
Article3. Robertson T, Fisher L. Prognostic significance of coronary artery aneurysm and ectasia in the Coronary Artery Surgery Study (CASS) registry. Prog Clin Biol Res. 1987. 250:325–339.4. Wong CK, Cheng CH, Lau CP, Leung WH. Asymptomatic congenital coronary artery aneurysm in adulthood. Eur Heart J. 1989. 10:947–949.
Article5. Chia HM, Tan KH, Jackson G. Non-atherosclerotic coronary artery aneurysms: two case reports. Heart. 1997. 78:613–616.
Article6. Demopoulos VP, Olympios CD, Fakiolas CN, Pissimissis EG, Economides NM, Adamopoulou E, et al. The natural history of aneurysmal coronary artery disease. Heart. 1997. 78:136–141.
Article7. Channon KM, Banning AP, Davies CH, Bashir Y. Coronary artery aneurysm rupture mimicking dissection of the thoracic aorta. Int J Cardiol. 1998. 65:115–117.
Article8. Hinterauer L, Roelli H, Goebel N, Steinbrunn W, Senning A. Huge left coronary artery aneurysm associated with multiple arterial aneurysms. Cardiovasc Intervent Radiol. 1985. 8:127–130.
Article9. Ghanta RK, Paul S, Couper GS. Successful revascularization of multiple coronary artery aneurysms using a combination of surgical strategies. Ann Thorac Surg. 2007. 84:e10–e11.10. Westaby S, Vaccari G, Katsumata T. Direct repair of giant right coronary aneurysm. Ann Thorac Surg. 1999. 68:1401–1403.11. Peterson MA, Monsein LH, Dangas G, Mehran R, Leon MB. Percutaneous transcatheter management of giant coronary aneurysms. Circulation. 1999. 100:E8–E11.
Article12. Assiri AS. Giant coronary artery aneurysm. Ann Saudi Med. 2000. 20:248–250.
Article13. Khositeseth A, Siripornpitak S, Pornkul R, Wanitkun S. Case report: Giant coronary aneurysm caused by Kawasaki disease: follow-up with echocardiography and multidetector CT angiography. Br J Radiol. 2008. 81:e106–e109.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Multiple Giant Coronary Aneurysms Arising from Coronary Fistula to the Pulmonary Artery Revealed in Aorta CT Angiography
- Right Coronary Artery to Left Ventricular Fistula with a Giant Right Coronary Artery Aneurysm: A case report
- Two Cases of Super-Giant Coronary Aneurysms after Kawasaki Disease
- CABG for Treating Unstable Angina with Multivessel Coronary Artery Aneurysms: A case report
- The Noninvasive Diagnosis and Postoperative Evaluation of Anomalous Right Coronary Artery from the Pulmonary Artery (ARCAPA) using Coronary MDCT: A Case Report
