Traumatic Neuroma around the Celiac Trunk after Gastrectomy Mimicking a Nodal Metastasis: A Case Report
- Affiliations
-
- 1Department of Diagnostic Radiology, Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. kjh2603@dsmc.or.kr
- 2Department of Surgery, Dongsan Medical Center, Keimyung University School of Medicine, Daegu , Korea.
- 3Department of Pathology, Dongsan Medical Center, Keimyung University School of Medicine, Daegu , Korea.
- KMID: 1779441
- DOI: http://doi.org/10.3348/kjr.2007.8.3.242
Abstract
- Traumatic neuroma is a well-known disorder that occurs after trauma or surgery involving the peripheral nerve and develops from a nonneoplastic proliferation of the proximal end of a severed, partially transected, or injured nerve. We present a case of traumatic neuroma around the celiac trunk after gastrectomy in a 56-year-old man, which was confirmed by pathology. CT demonstrated the presence of a lobulated, homogeneous, hypoattenuating mass around the celiac trunk, mimicking a nodal metastasis.
Keyword
MeSH Terms
Figure
-
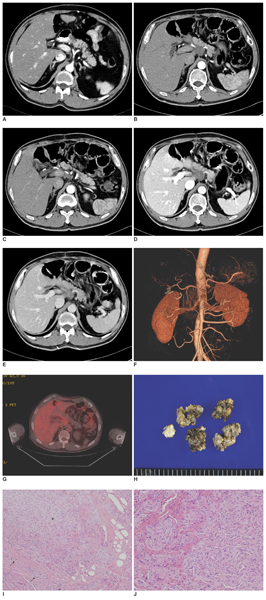
Fig. 1 A 56-year-old man with traumatic neuroma around the celiac trunk. A. A contrast-enhanced abdominal CT scan in the arterial phase showed no mass present around the celiac trunk 5 months previously. B, C. Contrast-enhanced abdominal CT scans in the arterial phase show a lobulated hypoattenuating soft tissue mass in the celiac region encasing the common hepatic artery, splenic artery, gastroduodenal artery, and the proper hepatic artery. D, E. Contrast-enhanced abdominal CT scans in the portal phase (D) and equilibrium phase (E) show a mild homogeneous enhancement of this mass. F. Volume-rendering CT angiography shows that the celiac trunk and its tributaries are patent without vessel wall irregularities, or vessel caliber stenosis. G. Fluorodeoxyglucose (FDG)-positron emission tomography (PET) image shows no increased uptake around the celiac trunk with a mean standardized uptake value of 3.2. H. The resected celiac mass is composed of several pieces of irregular pale tan to yellow firm tissue, measuring 3.5 × 3.0 × 1.0 cm in aggregates. I, J. Microscopically, the celiac mass consists of small (arrows) and large (asterisk) proliferating fascicles of nerve in a background of collagen and fat tissue (Hematoxylin & Eosin staining, × 100). The celiac mass is composed of a haphazard proliferation of nerve fascicles, including axons with their investitures of myelin, Schwann cells, and fibroblasts (Hematoxylin & Eosin staining, × 200).
Cited by 1 articles
-
Traumatic Neuroma at the Inferior Mesenteric Artery Stump after Rectal Cancer Surgery: A Case Report and Literature Review
Sung Mi Jeon, Jae Young Lee, Sun-Ju Byeon
Korean J Gastroenterol. 2016;68(5):279-283. doi: 10.4166/kjg.2016.68.5.279.
Reference
-
1. Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics. 1999. 19:1253–1280.2. Yabuuchi H, Kuroiwa T, Fukuya T, Tomita K, Hachitanda Y. Traumatic neuroma and recurrent lymphadenopathy after neck dissection: comparison of radiologic features. Radiology. 2004. 233:523–529.3. Nagata Y, Tomioka T, Chiba K, Kanematsu T. Traumatic neuroma of the common hepatic duct after laparoscopic cholecystectomy. Am J Gastroenterol. 1995. 90:1887–1888.4. Shimura K, Tamada K, Asada M, Watabiki N, Wada I, Tanaka N, et al. Intraductal ultrasonography of traumatic neuroma of the bile duct. Abdom Imaging. 2001. 26:632–634.5. van Gulik TM, Brumelkamp WH, Lygidakis NJ. Traumatic neuroma giving rise to biliary obstruction after reconstructive surgery for iatrogenic lesions of biliary tract-a report of three cases. Hepatogastroenterology. 1989. 36:255–257.6. Mentha G, Rubbia-Brandt L, Orci L, Becker C, Giostra E, Majno P, et al. Traumatic neuroma with biliary duct obstruction after orthotopic liver transplantation. Transplantation. 1999. 67:177–179.7. Katsinelos P, Dimiropoulos S, Galanis I, Tsolkas P, Paroutoglu G, Arvaniti M, et al. Biliary stricture due to neuroma after an innocent blunt abdominal trauma. Surg Endosc. 2002. 16:1494.8. Li H, Zeng MS, Zhou KR, Jin DY, Lou WH. Pancreatic adenocarcinoma: the different CT criteria for peripancreatic major arterial and venous invasion. J Comput Assist Tomogr. 2005. 29:170–175.9. Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, Chung JK, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 2006. 7:57–69.10. Chen J, Cheong JH, Yun MJ, Kim J, Lim JS, Hyung WJ, et al. Improvement in preoperative staging of gastric adenocarcinoma with positron emission tomography. Cancer. 2005. 103:2383–2390.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Neuroma at the Inferior Mesenteric Artery Stump after Rectal Cancer Surgery: A Case Report and Literature Review
- Unusual Presentation of Traumatic Neuroma of the Medial Plantar Nerve after Deep Laceration Mimicking a Foreign Body Granuloma: A Case Report
- A Traumatic Neuroma in Breast Cancer Patient after Mastectomy: A Case Report
- A Case of Neuroma Cutis
- Amputation Neuroma Mimicking Common Bile Duct Cancer: A Case Report
