Performance Assessment of the SOFA, APACHE II Scoring System, and SAPS II in Intensive Care Unit Organophosphate Poisoned Patients
- Affiliations
-
- 1Department of Emergency Medicine, Samsung Changwon Hospital, Sungkyunkwan University School of Medicine, Changwon, Korea. galjoun@hanmail.net
- 2Department of Emergency Medicine, Bundang Jesaeng General Hospital, Seongnam, Korea.
- 3Department of Emergency Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, Korea.
- 4Department of Emergency Medicine, Inje University College of Medicine, Busan, Korea.
- KMID: 1779426
- DOI: http://doi.org/10.3346/jkms.2013.28.12.1822
Abstract
- This study assessed the ability of the Sequential Organ Failure Assessment (SOFA) and Acute Physiology, Chronic Health Evaluation (APACHE) II scoring systems, as well as the Simplified Acute Physiology Score (SAPS) II method to predict group mortality in intensive care unit (ICU) patients who were poisoned with organophosphate. The medical records of 149 organophosphate poisoned patients admitted to the ICU from September 2006 to December 2012 were retrospectively examined. The SOFA, APACHE II, and SAPS II were calculated based on initial laboratory data in the Emergency Department, and during the first 24 hr of ICU admission. The probability of death was calculated for each patient based on the SOFA score, APACHE II score, and SAPS II equations. The ability to predict group mortality by the SOFA score, APACHE II score, and SAPS II method was assessed using two by two decision matrices and receiver operating characteristic (ROC) curve analysis. A total of 131 patients (mean age, 61 yr) were enrolled. The sensitivities, specificities, and accuracies were 86.2%, 82.4%, and 83.2% for the SOFA score, respectively; 65.5%, 68.6%, and 67.9% for the APACHE II scoring system, respectively; and 86.2%, 77.5%, and 79.4% for the SAPS II, respectively. The areas under the curve in the ROC curve analysis for the SOFA score, APACHE II scoring system, and SAPS II were 0.896, 0.716, and 0.852, respectively. In conclusion, the SOFA, APACHE II, and SAPS II have different capability to discriminate and estimate early in-hospital mortality of organophosphate poisoned patients. The SOFA score is more useful in predicting mortality, and easier and simpler than the APACHE II and SAPS II.
MeSH Terms
Figure
-

Fig. 1 Organophosphate poisoned patients between September 2008 and February 2013.
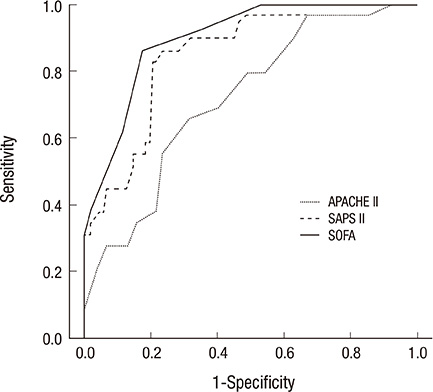
Fig. 2 Receiver operating curves for predicting death according the Sequential Organ Failure Assessment (SOFA), Acute Physiology and Chronic Health Evaluation (APACHE) II, and Simplified Acute Physiology Score (SAPS) II scoring systems. The areas under the curve and 95% confidence intervals for these indicators were 0.896 (0.839-0.954) for SOFA, 0.716 (0.615-0.817) for APACHE II, and 0.852 (0.780-0.923) for SAPS II, respectively.
Cited by 2 articles
-
Characteristics and Prognosis of Hospitalized Patients at High Risk of Deterioration Identified by the Rapid Response System: a Multicenter Cohort Study
Sang Hyuk Kim, Ji Young Hong, Youlim Kim
J Korean Med Sci. 2021;36(32):e235. doi: 10.3346/jkms.2021.36.e235.Acute Physiologic and Chronic Health Examination II and Sequential Organ Failure Assessment Scores for Predicting Outcomes of Out-of-Hospital Cardiac Arrest Patients Treated with Therapeutic Hypothermia
Sung Joon Kim, Yong-Su Lim, Jin Seong Cho, Jin Joo Kim, Won Bin Park, Hyuk Jun Yang
Korean J Crit Care Med. 2014;29(4):288-296. doi: 10.4266/kjccm.2014.29.4.288.
Reference
-
1. Jeyaratnam J. Acute pesticide poisoning: a major global health problem. World Health Stat Q. 1990; 43:139–144.2. Senanayake N, Karalliedde L. Neurotoxic effects of organophosphorus insecticides: an intermediate syndrome. N Engl J Med. 1987; 316:761–763.3. Nouira S, Abroug F, Elatrous S, Boujdaria R, Bouchoucha S. Prognostic value of serum cholinesterase in organophosphate poisoning. Chest. 1994; 106:1811–1814.4. Tsao TC, Juang YC, Lan RS, Shieh WB, Lee CH. Respiratory failure of acute organophosphate and carbamate poisoning. Chest. 1990; 98:631–636.5. Eddleston M, Gunnell D, Karunaratne A, de Silva D, Sheriff MH, Buckley NA. Epidemiology of intentional self-poisoning in rural Sri Lanka. Br J Psychiatry. 2005; 187:583–584.6. Sidell FR, Borak J. Chemical warfare agents: II. nerve agents. Ann Emerg Med. 1992; 21:865–871.7. Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North American Multicenter Study. JAMA. 1993; 270:2957–2963.8. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure: on behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996; 22:707–710.9. Hargrove J, Nguyen HB. Bench-to-bedside review: outcome predictions for critically ill patients in the emergency department. Crit Care. 2005; 9:376–383.10. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985; 13:818–829.11. Vassar MJ, Wilkerson CL, Duran PJ, Perry CA, Holcroft JW. Comparison of APACHE II, TRISS, and a proposed 24-hour ICU point system for prediction of outcome in ICU trauma patients. J Trauma. 1992; 32:490–499.12. Hosmer DW, Lemeshow S. Applied logistic regression. 2nd ed. New York: Wiley;2000.13. Tran DD, Groeneveld AB, van der Meulen J, Nauta JJ, Strack van Schijndel RJ, Thijs LG. Age, chronic disease, sepsis, organ system failure, and mortality in a medical intensive care unit. Crit Care Med. 1990; 18:474–479.14. Deitch EA. Multiple organ failure: pathophysiology and potential future therapy. Ann Surg. 1992; 216:117–134.15. Knaus WA, Wanger DP, Draper EA. Relationship between acute physiologic derangement and risk of death. J Chronic Dis. 1985; 38:295–300.16. Wilson RF, Gibson D, Percinel AK, Ali MA, Baker G, LeBlanc LP, Lucas C. Severe alkalosis in critically ill surgical patients. Arch Surg. 1972; 105:197–203.17. Shoemaker WP, Chang P, Czer L, Bland R, Shabot MM, State D. Cardiorespiratory monitoring in postoperative patients: I. prediction of outcome and severity of illness. Crit Care Med. 1979; 7:237–242.18. Kim H, Han SB, Kim JS, Lee MJ, Park JS, Kwon WY, Eo EK, Oh BJ, Lee SW, Suh JH, et al. Clinical implication of acetylcholinesterase in acute organophosphate poisoning. J Korean Soc Clin Toxicol. 2008; 6:25–31.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Physiology and Chronic Health Evaluation II Score and Sequential Organ Failure Assessment Score as Predictors for Severe Trauma Patients in the Intensive Care Unit
- Performance of the PSS, APACHE II, and SOFA score as in-hospital prognostic tool in glufosinate-poisoned patients in the intensive care unit
- Intensive Care National Audit & Research Centre Model for Predicting 1-Month Mortality in Emergency Intensive Care Unit Korean Patients
- Performance of APACHE IV in Medical Intensive Care Unit Patients: Comparisons with APACHE II, SAPS 3, and MPMâ‚€ III
- The Clinical Efficacy of GOCA Scoring System in Patients with Acute Respiratory Distress Syndrome
