J Korean Med Sci.
2009 Jun;24(3):513-516. 10.3346/jkms.2009.24.3.513.
A Case of Successful Selective Abortion Using Radio-frequency Ablation in Twin Pregnancy Suffering from Severe Twin to Twin Transfusion Syndrome
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Mokdong Ewha Medical Center, School of Medicine, Ewha Womans University, Seoul, Korea. ewhapmh@yahoo.com
- KMID: 1779173
- DOI: http://doi.org/10.3346/jkms.2009.24.3.513
Abstract
- Twin to twin transfusion syndrome (TTTS) is one of the major complication of monochorionic twin pregnancy which is mainly understood by placental vascular anastomosis. Perinatal mortality and morbidity is high as 80-100% if untreated and even higher if the disease is developed at early stage. Variety of methods of isolating or intercepting placental vascular anastomosis are introduced, but they are only available in centers where all the required equipments are prepared. We report here a case of TTTS complicated with severe polyhydroamnios during the second trimester. The blood supply to donor twin was interrupted successfully at 19+2 weeks of gestation by minimally invasive radio-frequency cord ablation, under ultrasound guidance. The normal recipient twin was delivered successfully at 35 weeks of gestation and had no eventful neonatal course.
MeSH Terms
Figure
-

Fig. 1 Echogenic lesion in umbilical cord during radio-frequency cord ablation procedure (arrows represent electrodes).
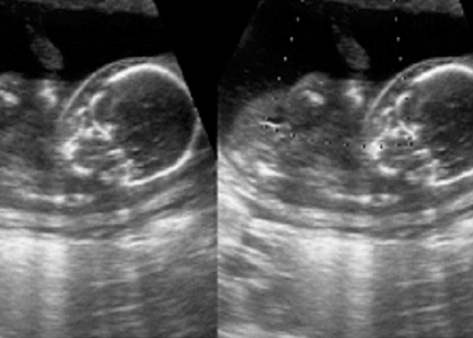
Fig. 2 Absent blood flow in the umbilical cord of the 2nd twin after radio-frequency cord ablation.

Fig. 3 Mild ventriculomegaly of surviving 1st fetus at 24+6 weeks of gestation.
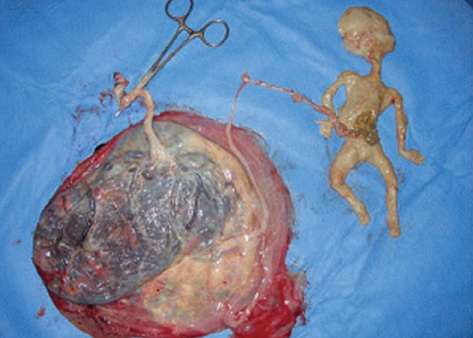
Fig. 4 Findings of selectively terminated 2nd fetus after delivery at 35 weeks of gestation. Iatrogenic gastroschisis and mono-chorionic twin placenta of pregnancy are seen.
Reference
-
1. Huber A, Hecher K. How we can diagnose and manage twin-twin transfusion syndrome. Best Pract Res Clin Obstet Gynaecol. 2004. 18:543–556.2. Wee LY, Fisk NM. The twin-twin transfusion syndrome. Semin Neonatol. 2002. 7:187–202.
Article3. van Gemert MJ, Umur A, Tijssen JG, Ross MG. Twin-twin transfusion syndrome: etiology, severity and rational management. Curr Opin Obstet Gynecol. 2001. 13:193–206.
Article4. Brennan JN, Diwan RV, Rosen MG, Bellon EM. Fetofetal transfusion syndrome: prenatal ultrasonographic diagnosis. Radiology. 1982. 143:535–536.
Article5. Vetter K. Considerations on growth discordant twins. J Perinat Med. 1993. 21:267–272.
Article6. Tan TY, Taylor MJ, Wee LY, Vanderheyden T, Wimalasundera R, Fisk NM. Doppler for artery-artery anastomosis and stage-independent survival in twin-twin transfusion. Obstet Gynecol. 2004. 103:1174–1180.
Article7. Blickstein I. The twin-to-twin transfusion syndrome. Obstet Gynecol. 1990. 76:714–721.8. Urig MA, Clewell WH, Elliott JP. Twin-twin transfusion syndrome. Am J Obstet Gynecol. 1990. 163:1522–1526.
Article9. Quintero RA, Morales WJ, Allen MH, Bornick PW, Johnson PK, Kruger M. Staging of twin-twin transfusion syndrome. J Perinatol. 1999. 19:550–555.
Article10. Saunders NJ, Snijders RJ, Nicolaides KH. Therapeutic amniocentesis in twin-twin transfusion syndrome appearing in the second trimester of pregnancy. Am J Obstet Gynecol. 1992. 166:820–824.
Article11. Quintero RA, Comas C, Bornick PW, Allen MH, Kruger M. Selective versus non-selective laser photocoagulation of placental vessels in twin-to-twin transfusion syndrome. Ultrasound Obstet Gynecol. 2000. 16:230–236.
Article12. Lemery DJ, Vanlieferinghen P, Gasq M, Finkeltin F, Beaufrere AM, Bey tout M. Fetal umbilical cord ligation under ultrasound guidance. Ultrasound Obstet Gynecol. 1994. 4:399–401.
Article13. De Lia JE, Cruikshank DP, Keye WR Jr. Fetoscopic neodymium: yag laser occlusion of placental vessels in severe twin-twin transfusion syndrome. Obstet Gynecol. 1990. 75:1046–1053.
Article14. Quintero RA, Dickinson JE, Morales WJ, Bornick PW, Bermúdez C, Cincotta R, Chan FY, Allen MH. Stage-based treatment of twin-twin transfusion syndrome. Am J Obstet Gynecol. 2003. 188:1333–1340.
Article15. Hecher K, Plath H, Bregenzer T, Hansmann M, Hackeloer BJ. Endoscopic laser surgery versus serial amniocentesis in the treatment of severe twin-twin transfusion syndrome. Am J Obstet Gynecol. 1999. 180:717–724.16. Mari G, Roberts A, Detti L, Kovanci E, Stefos T, Bahado-Singh RO, Deter RL, Fisk NM. Perinatal morbidity and mortality rates in severe twin-twin transfusion syndrome: results of the International Amnioreduction Registry. Am J Obstet Gynecol. 2001. 185:708–715.
Article17. Golbus MS, Cunningham N, Goldberg JD, Anderson R, Filly R, Callen P. Selective termination of multiple gestations. Am J Med Genet. 1988. 31:339–348.
Article18. Sydorak RM, Feldstein V, Machin G, Tsao K, Hirose S, Lee H, Farmer DL, Harrison MR, Albanese CT. Fetoscopic treatment for Discordant twins. J Pediatr Surg. 2002. 37:1736–1739.
Article19. Denbow ML, Overton TG, Duncan KR, Cox PM, Fisk NM. High failure rate of umbilical vessel occlusion by ultrasound-guided injection of absolute alcohol or enbucrilate gel. Prenat Diagn. 1999. 19:527–532.
Article20. Morel O, Tran N, Marchal F, Hennequin V, Foliguet B, Villemot JP, Thiebaugeorges O. Ultrasound-guided radiofrequency-driven umbilical cord occlusion: an in-vitro study. Ultrasound Obstet Gynecol. 2006. 28:187–192.21. Spadola AC, Simpson LL. Selective termination procedures in monochorionic pregnancies. Semin Perinatol. 2005. 29:330–337.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Twin-twin transfusion syndrome; TTTS
- Twin-to-Twin Transfusion Syndrome: Diagnosis and Managements
- A case of antenatal periventricular leukomalacia in monochorionic twin pregnancy complicated with twin-to-twin transfusion syndrome
- Selective Termination Procedures in Monochorionic Pregnancies
- A cass of Twin to Twin Transfusion Syndrome
