ANCA-Negative Wegener's Granulomatosis with Multiple Lower Cranial Nerve Palsies
- Affiliations
-
- 1Department of Neurology, Ewha Womans University School of Medicine and Ewha Medical Research Institute, Seoul, Korea. jjeong@ewha.ac.kr
- 2Department of Otolaryngology, Ewha Womans University School of Medicine and Ewha Medical Research Institute, Seoul, Korea.
- 3Department of Pathology, Ewha Womans University School of Medicine and Ewha Medical Research Institute, Seoul, Korea.
- KMID: 1777672
- DOI: http://doi.org/10.3346/jkms.2013.28.11.1690
Abstract
- Wegener's granulomatosis (WG) is a systemic vasculitis affecting small and medium-sized vessels with granulomatous formation. Though it is known for respiratory tract and kidney involvement, neurologic manifestation has been also reported. Herein we report a patient who suffered pansinusitis with multiple lower cranial nerve palsies but reached remission by immunosuppressant after the diagnosis of WG. A 54-yr-old female visited with headache, hearing difficulty, and progressive bulbar symptoms. She experienced endoscopic sinus surgeries due to refractory sinusitis. Neurologic examination revealed multiple lower cranial nerve palsies. Vasculitic markers showed no abnormality. Nasal biopsy revealed granulomatous inflammation and vasculitis involving small vessels. Given cyclophosphamide and prednisolone, her symptoms were prominently improved. WG should be considered in the patient with multiple cranial nerve palsies, especially those with paranasal sinus disease. Because WG can be lethal if delayed in treatment, prompt immunosuppressant is warranted after the diagnostic tissue biopsy.
MeSH Terms
-
Anti-Inflammatory Agents/therapeutic use
Antibodies, Antineutrophil Cytoplasmic
Antineoplastic Agents, Alkylating/therapeutic use
Cranial Nerve Diseases/*diagnosis/drug therapy/radionuclide imaging
Cyclophosphamide/therapeutic use
Diagnosis, Differential
Female
Humans
Middle Aged
Prednisolone/therapeutic use
Sinusitis/surgery
Vasculitis
Wegener Granulomatosis/*diagnosis/drug therapy/radionuclide imaging
Anti-Inflammatory Agents
Antibodies, Antineutrophil Cytoplasmic
Antineoplastic Agents, Alkylating
Cyclophosphamide
Prednisolone
Figure
-
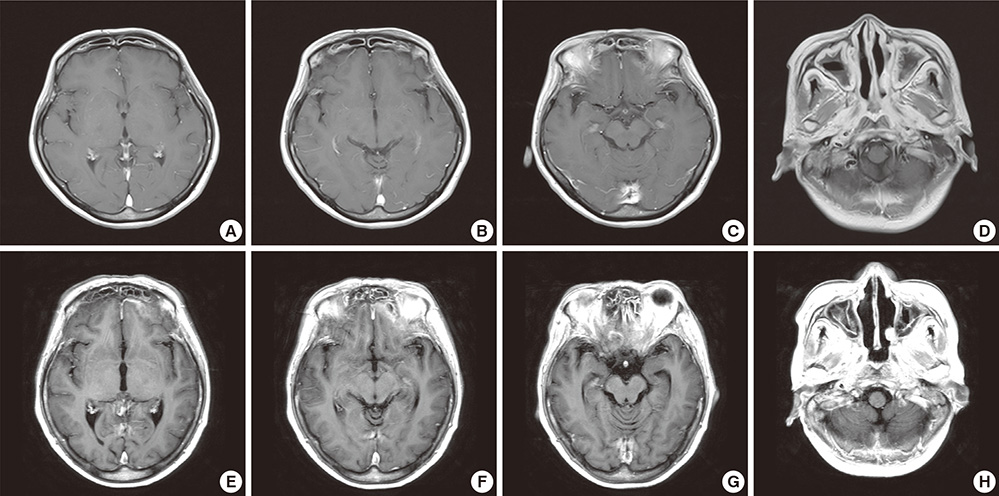
Fig. 1 Brain MRI. (A to D) The first MRI. Initial outside brain MRI was not remarkable, except bilateral mastoiditis and extensive sinusitis. (E to H) The second MRI. Repeated brain MRI after 5 months shows new meningeal thickening with enhancement around the tentorium cerebelli, inferior aspect of frontotemporal lobe adjacent to sinuses and nasopharynx. Also diffuse sinusitis in bilateral frontal, ethmoid, sphenoid, and maxillary sinuses were still existed.

Fig. 2 Neck CT. (A to C) Quite extensive sinusitis expanding to orbit and retromaxillary fat pad is observed. Note that massive swollen lesions of nasopharynx with positive enhancement penetrated the skull base.

Fig. 3 18F-FDG PET. (A to C) Prominent hypermetabolism in bilateral tonsil area of nasopharynx and multiple lymph nodes of neck level II and III were shown. (D-F) Multiple sinusitis were also demonstrated as hypermetabolic lesions. 18F-FDG PET: 18F-fluorodeoxyglucose positron-emission tomography.

Fig. 4 Nasopharygenal biopsy. (A) The nasopharyngeal tissue shows dense polymorphous inflammatory cell infiltrates composed of mature lymphocytes, plasma cells, histiocytes, eosinophils and neutrophils. There are few multinucleated giant cells which represent granulomatous component of the disease. (B) Granulomatous inflammation involving vessel wall and lumen (vasculitis) with necrosis is evident.
Reference
-
1. Martinez Del Pero M, Sivasothy P. Vasculitis of the upper and lower airway. Best Pract Res Clin Rheumatol. 2009; 23:403–417.2. Rodrigues CE, Callado MR, Nobre CA, Moura FE, Vieira RM, de Albuquerque LA, Vieira WP. Wegener's granulomatosis: prevalence of the initial clinical manifestations: report of six cases and review of the literature. Rev Bras Reumatol. 2010; 50:150–164.3. Cattaneo L, Chierici E, Pavone L, Grasselli C, Manganelli P, Buzio C, Pavesi G. Peripheral neuropathy in Wegener's granulomatosis, Churg-Strauss syndrome and microscopic polyangiitis. J Neurol Neurosurg Psychiatry. 2007; 78:1119–1123.4. Pagnoux C, Wolter NE. Vasculitis of the upper airways. Swiss Med Wkly. 2012; 142:w13541.5. Nishino H, Rubino FA, DeRemee RA, Swanson JW, Parisi JE. Neurological involvement in Wegener's granulomatosis: an analysis of 324 consecutive patients at the Mayo Clinic. Ann Neurol. 1993; 33:4–9.6. Armani M, Spinazzi M, Andrigo C, Fassina A, Mantovan M, Tavolato B. Severe dysphagia in lower cranial nerve involvement as the initial symptom of Wegener's granulomatosis. J Neurol Sci. 2007; 263:187–190.7. Murphy JM, Gomez-Anson B, Gillard JH, Antoun NM, Cross J, Elliott JD, Lockwood M. Wegener granulomatosis: MR imaging findings in brain and meninges. Radiology. 1999; 213:794–799.8. Kodama S, Nomi N, Suzuki M. Wegener's granulomatosis with extensive bone abnormalities mimicking fungal sinusitis. Case Rep Otolaryngol. 2012; 2012:103403.9. Kashiyama T, Suzuki A, Mizuguchi K. Wegener's granulomatosis with multiple cranial nerve involvements as the initial clinical manifestations. Intern Med. 1995; 34:1110–1113.10. Spísek R, Kolouchová E, Jensovský J, Rusina R, Fendrych P, Plas J, Bartůnková J. Combined CNS and pituitary involvement as a primary manifestation of Wegener granulomatosis. Clin Rheumatol. 2006; 25:739–742.11. Akahoshi M, Yoshimoto G, Nakashima H, Miyake K, Inoue Y, Tanaka Y, Tsukamoto H, Horiuchi T, Otsuka T, Harada M. MPO-ANCA-positive Wegener's granulomatosis presenting with hypertrophic cranial pachymeningitis: case report and review of the literature. Mod Rheumatol. 2004; 14:179–183.12. Warnatz K, Peter HH, Schumacher M, Wiese L, Prasse A, Petschner F, Vaith P, Volk B, Weiner SM. Infectious CNS disease as a differential diagnosis in systemic rheumatic diseases: three case reports and a review of the literature. Ann Rheum Dis. 2003; 62:50–57.13. Allen SD, Harvey CJ. Imaging of Wegener's granulomatosis. Br J Radiol. 2007; 80:757–765.14. Del Buono EA, Flint A. Diagnostic usefulness of nasal biopsy in Wegener's granulomatosis. Hum Pathol. 1991; 22:107–110.15. Madhira S, Hamid QA, Prayaga SM, Kolloju S. Limited Wegener's granulomatosis with predominant otological presentation. Indian J Otolaryngol Head Neck Surg. 2011; 63:4–5.16. Müller S, Eljack S, DelGaudio JM. Clinical pathologic conference case 1: Wegener's granulomatosis. Head Neck Pathol. 2011; 5:268–272.17. Agarwal PK, Gogia A. Limited Wegener's granulomatosis with p-ANCA positivity. J Indian Acad Clin Med. 2004; 5:348–350.18. Said MS. Upper respiratory tract symptoms, renal involvement and vasculitis: a case report and review of wegener granulomatosis. J Clin Med Res. 2010; 2:189–193.19. Swain S, Ray R. Wegener's granulomatosis of nose: a case report. Indian J Otolaryngol Head Neck Surg. 2011; 63:402–404.20. Langford CA. Cyclophosphamide as induction therapy for Wegener's granulomatosis and microscopic polyangiitis. Clin Exp Immunol. 2011; 164:31–34.21. Daderian AD, Chayasirisobhon S. An unusual case of multiple cranial nerve palsies in Wegener's granulomatosis. J Natl Med Assoc. 2000; 92:455–457.22. Nordmark G, Boquist L, Rönnblom L. Limited Wegener's granulomatosis with central nervous system involvement and fatal outcome. J Intern Med. 1997; 242:433–436.23. Nowack R, Wachtler P, Kunz J, Rasmussen N. Cranial nerve palsy in Wegener's granulomatosis: lessons from clinical cases. J Neurol. 2009; 256:299–304.24. Loke YK, Tan MH. An unusual case of Wegener's granulomatosis. Med J Malaysia. 1998; 53:107–109.25. Langford CA, Talar-Williams C, Barron KS, Sneller MC. A staged approach to the treatment of Wegener's granulomatosis: induction of remission with glucocorticoids and daily cyclophosphamide switching to methotrexate for remission maintenance. Arthritis Rheum. 1999; 42:2666–2673.26. Langford CA. Wegener's granulomatosis: current and upcoming therapies. Arthritis Res Ther. 2003; 5:180–191.27. Stone JH, Merkel PA, Spiera R, Seo P, Langford CA, Hoffman GS, Kallenberg CG, St Clair EW, Turkiewicz A, Tchao NK, et al. RAVE-ITN Research Group. Rituximab versus cyclophosphamide for ANCA-associated vasculitis. N Engl J Med. 2010; 363:221–232.28. Hermann J, Reittner P, Scarpatetti M, Graninger W. Successful treatment of meningeal involvement in Wegener's granulomatosis with infliximab. Ann Rheum Dis. 2006; 65:691–692.29. Just SA, Knudsen JB, Nielsen MK, Junker P. Wegener's granulomatosis presenting with pachymeningitis: clinical and imaging remission by rituximab. ISRN Rheumatol. 2011; 2011:608942.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- ANCA-negative limited Wegener's granulomatosis
- A Case of ANCA-Negative Generalized Wegener's Granulomatosis
- Facial Palsy as a Presenting Symptom of Wegener's Granulomatosis
- A case of Wegener's granulomatosis complicated by non-small cell lung cancer
- A Case of Limited form of Wegener's Granulomatosis in a Child
