Diagnosis of Recurrent Uterine Cervical Cancer: Computed Tomography versus Positron Emission Tomography
- Affiliations
-
- 1Department of Diagnostic Radiology, Korea Cancer Center Hospital, Seoul, Korea.
- KMID: 1777296
- DOI: http://doi.org/10.3348/kjr.2000.1.1.51
Abstract
OBJECTIVE
To determine the accuracy of CT and positron emission tomography (PET) in the diagnosis of recurrent uterine cervical cancer. MATERIALS AND METHODS: Imaging findings of CT and PET in 36 patients (mean age, 53 years) in whom recurrent uterine cervical cancer was suspected were analyzed retrospectively. Between October 1997 and May 1998, they had undergone surgery and/or radiation therapy. Tumor recurrence was confirmed by pathologic examination or follow-up studies. RESULTS: In detecting recurrent uterine cervical cancer, the sensitivity, specificity, and accuracy of CT were 77.8%, 83.3%, and 80.5%, respectively, while for PET, the corresponding figures were 100%, 94.4%, and 97.2%. The Chisquare test revealed no significant difference in specificity (p = .2888), but significant differences in sensitivity (p = .0339) and accuracy (p = .0244). CONCLUSION: PET proved to be a reliable screening method for detecting recurrent uterine cervical cancer, but to determine the anatomical localization of recurrent tumors, and thus decide an adequate treatment plan, CT was eventually needed.
Keyword
MeSH Terms
-
Adult
Cervix Neoplasms/*radiography/*radionuclide imaging
Comparative Study
Contrast Media
Female
Fludeoxyglucose F 18/diagnostic use
Human
Middle Age
Neoplasm Recurrence, Local/*radiography/*radionuclide imaging
Radiopharmaceuticals/diagnostic use
Sensitivity and Specificity
*Tomography, Emission-Computed
*Tomography, X-Ray Computed
Figure
-
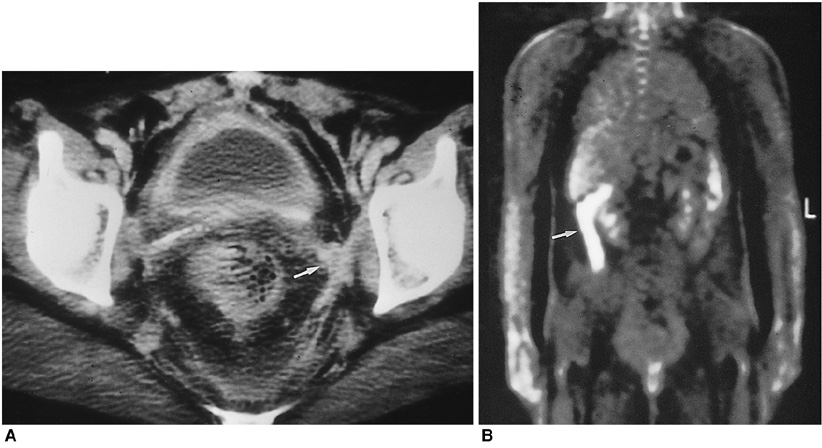
Fig. 1 A 39-year-old woman who had undergone radical hysterectomy due to uterine cervical carcinoma. A. Enhanced CT scan shows soft tissue mass on the left pelvic side wall (arrow). B. PET scan shows no hypermetabolic site in the pelvis. Since no interval change was seen during follow-up study, we concluded that this was a case of postoperative fibrosis. The highly metabolic lesion in left abdomen (arrow) is due to artifactual accumulation of FDG in ascending colon.
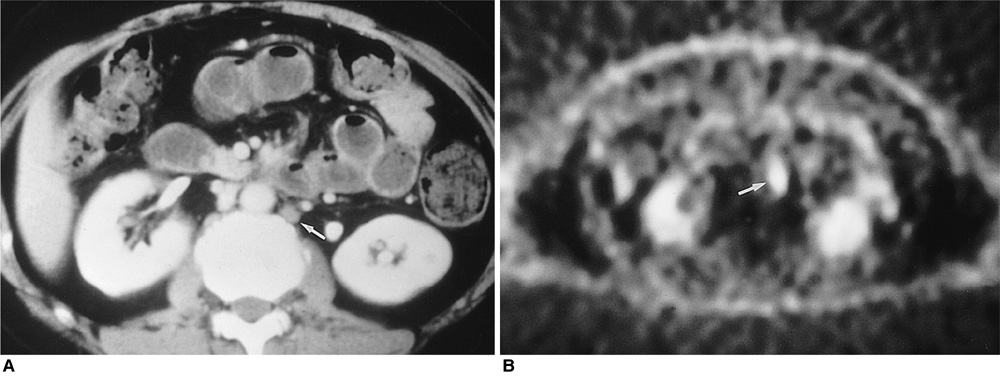
Fig. 2 A 52-year-old woman who had undergone radiation therapy due to uterine cervical cancer. A. Enhanced CT scan shows lymph node smaller than 1cm in the para-aortic area (arrow). B. PET scan shows hypermetabolic area (SUV = 3.8 ml/kg) in the para-aortic chain (arrow).
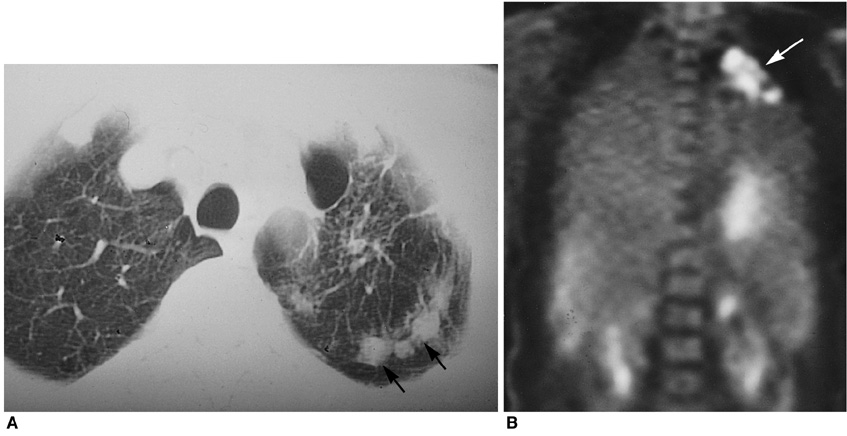
Fig. 3 A 41-year-old woman with uterine cervical cancer. False positive PET scan due to pulmonary tuberculosis. A. CT scan shows multiple nodules in left upper lung (arrows). B. PET scan shows hypermetabolic lesion (SUV = 9.6 ml/kg) in left upper lung (arrow). Tuberculosis was confirmed by polymerase chain reaction of the sputum.
Reference
-
1. Halpin TF, Frick HC, Munnell EW. Critical points of failure in the therapy of cancer of the cervix: a reappraisal. Am J Obstet Gynecol. 1972. 114:755–764.2. Walsh JW, Amendola MA, Hall DJ, Tisnado J, Goplerud DR. Recurrent carcinoma of the cervix: CT diagnosis. AJR. 1981. 136:117–122.3. Cunningham JJ, Fuks ZY, Castellino RA. Radiographic manifestations of carcinoma of the cervix and complications of its treatment. Radiol Clin North Am. 1974. 12:93–108.4. Weber TM, Sostman HD, Spritzer CE, et al. Cervical carcinoma: determination of recurrent tumor extent versus radiation changes with MR imaging. Radiology. 1995. 194:135–139.5. Hricak H, Swift PS, Campos Z, Quivey JM, Gildengorin V, Goranson H. Irradiation of the cervix uteri: value of unenhanced and contrast-enhanced MR imaging. Radiology. 1993. 189:381–388.6. Williams MP, Husband JE, Heron CW, Cherryman GR, Koslin DB. Magnetic resonance imaging in recurrent carcinoma of the cervix. Br J Radiol. 1989. 62:544–550.7. Flueckiger F, Ebner F, Poschauko H, Tamussino K, Einspieler R, Ranner G. Cervical cancer: serial MR imaging before and after primary radiation therapy-a 2-year follow-up study. Radiology. 1992. 184:89–93.8. Di Chiro G. Positron emission tomography using [18F]fluorodeoxyglucose in brain tumors-a powerful diagnostic and prognostic tool. Invest Radiol. 1988. 22:360–371.9. Carlson V, Delclos L, Fletcher GH. Distant metastases in squamous-cell carcinoma of the uterine cervix. Radiology. 1967. 88:961–966.10. Keettel WC, Van Voorhis LW, Latourette HB. Management of recurrent carcinoma of the cervix. Am J Obstet Gynecol. 1968. 102:671–677.11. Hoh CK, Schiepers C, Seltzer MA, et al. PET in oncology: will it replace the other modalities? Semin Nucl Med. 1997. 27:94–106.12. Anzai Y, Carroll WR, Quint DJ, et al. Recurrence of head and neck cancer after surgery or irradiation: prospective comparison of 2-deoxy-2-[F-18]fluoro-D-glucose PET and MR imaging diagnoses. Radiology. 1996. 200:135–141.13. Bender H, Kirst J, Palmedo H, et al. Value of 18-fluoro-deoxyglucose positron emission tomography in the staging of recurrent breast carcinoma. Anticancer Res. 1997. 17:1687–1692.14. Budinger TF, Brennan KM, Moses WW, Derenzo SE. Advances in positron tomography for oncology. Nucl Med Biol. 1996. 23:659–667.15. Blahd WH, Brown CV, Khonsary SA, et al. PET scans of abdominal malignancy. World J Surg. 1996. 20:245–247.16. Delbeke D, Martin WH, Sandler MP, Chapman WC, Wright JK Jr, Pinson CW. Evaluation of benign vs malignant hepatic lesions with positron emission tomography. Arch Surg. 1998. 133:510–516.17. Haseman MK, Reed NL, Rosenthal SA. Monoclonal antibody imaging of occult prostate cancer in patients with elevated prostate-specific antigen. Positron emission tomography and biopsy correlation. Clin Nucl Med. 1996. 21:704–713.18. McGuirt WF, Greven KM, Keyes JW Jr, Williams DW 3rd, Watson N. Laryngeal radionecrosis versus recurrent cancer: a clinical approach. Ann Otol Rhinol Laryngol. 1998. 107:293–296.19. Miraldi F, Vesselle H, Faulhaber PF, Adler LP, Leisure GP. Elimination of artifactual accumulation of FDG in PET imaging of colorectal cancer. Clin Nucl Med. 1998. 23:3–7.20. Ogunbiyi OA, Flanagan FL, Dehdashti F, et al. Detection of recurrent and metastatic colorectal cancer: comparison of positron emission tomography and computed tomography. Ann Surg Oncol. 1997. 4:613–620.21. Greven KM, Williams DW 3rd, Keyes JW Jr, McGuirt WF, Watson NE Jr, Case LD. Can positron emission tomography distinguish tumor recurrence from irradiation sequelae in patients treated for larynx cancer? Cancer J Sci Am. 1997. 3:353–357.22. Garner CM. Positron emission tomography: new hope for early detection of recurrent brain tumors. Cancer Nurs. 1997. 20:277–284.23. Schiepers C. Role of positron emission tomography in the staging of lung cancer. Lung Cancer. 1997. 17(1):S. 29–35.24. Simon GH, Nitzsche EU, Laubenberger JJ, Einert A, Moser E. PET imaging of recurrent medullary thyroid cancer. Nuklearmedizin. 1996. 35:102–104.25. Keogan MT, Lowe VJ, Baker ME, McDermott VG, Lyerly HK, Coleman RE. Local recurrence of rectal cancer: evaluation with F-18 fluorodeoxyglucose PET imaging. Abdom Imaging. 1997. 22:332–337.26. Hudgins PA, Burson JG, Gussack GS, Grist WJ. CT and MR appearance of recurrent malignant head and neck neoplasms after resection and flap reconstruction. AJNR. 1994. 15:1689–1694.27. Vesselle HJ, Miraldi FD. FDG PET of the retroperitoneum: normal anatomy, variants, pathologic conditions, and strategies to avoid diagnostic pitfalls. RadioGraphics. 1998. 18:805–823.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- PET Imaging for Gynecologic Malignancy
- Unusual Peritoneal Metastasis of Late Recurrent Uterine Cervical Cancer: A Case Report and Literature Review
- 18F-2-Deoxy-2-Fluoro-D-Glucose Positron Emission Tomography: Computed Tomography for Preoperative Staging in Gastric Cancer Patients
- The role of positron emission tomography in the diagnosis and management of gynecologic malignancies
- Advances in diagnosis and treatment of metastatic cervical cancer
