Migrating Lobar Atelectasis of the Right Lung: Radiologic Findings in Six Patients
- Affiliations
-
- 1Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 1777293
- DOI: http://doi.org/10.3348/kjr.2000.1.1.33
Abstract
OBJECTIVE
To describe the radiologic findings of migrating lobar atelectasis of the right lung. MATERIALS AND METHODS: Chest radiographs (n = 6) and CT scans (n = 5) of six patients with migrating lobar atelectasis of the right lung were analyzed retrospectively. The underlying diseases associated with lobar atelectasis were bron-chogenic carcinoma (n = 4), bronchial tuberculosis (n = 1), and tracheobronchial amyloidosis (n = 1). RESULTS: Atelectasis involved the right upper lobe (RUL) (n = 3) and both the RUL and right middle lobe (RML) (n = 3). On supine anteroposterior radiographs (n = 5) and on an erect posteroanterior radiograph (n = 1), the atelectatic lobe(s) occupied the right upper lung zone, with a wedge shape abutting onto the right mediastinal border. On erect posteroanterior radiographs (n = 6), the heavy atelectatic lobe(s) migrated downward, forming a perior infrahilar area of increased opacity and obscuring the right cardiac margin. Erect lateral radi-ographs (n = 4) showed inferior shift of the anterosuperiorly located atelectatic lobe(s) to the anteroinferior portion of the hemithorax. CONCLUSION: Atelectatic lobe(s) can move within the hemithorax according to changes in a patient's position. This process involves the RUL or both the RUL and RML.
Keyword
MeSH Terms
Figure
-
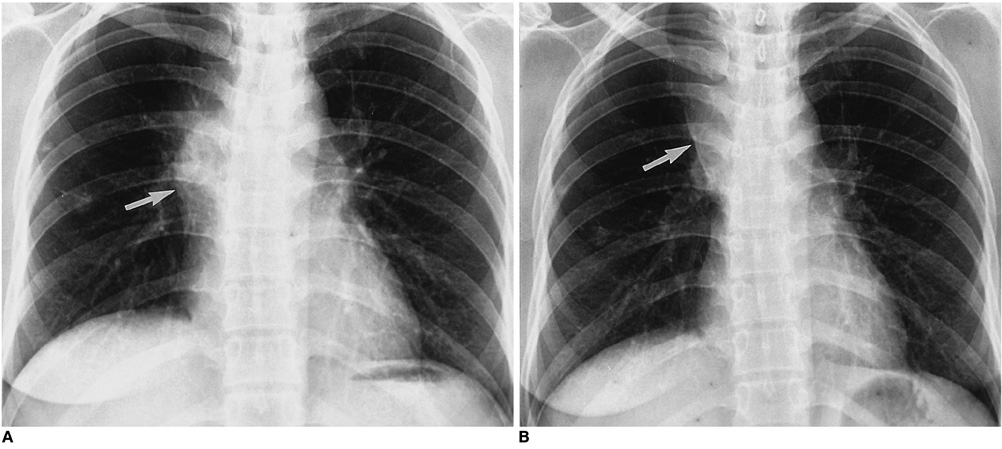
Fig. 1 Migrating right upper lobar atelectasis caused by tuberculous bronchostenosis in a 29-year-old female. A. Erect posteroanterior chest radiograph obtained on admission shows increased opacity in the right hilar area obscuring the right cardiac margin (arrow). B. Erect posteroanterior radiograph obtained two days later shows migration of the opacity to upper lung zone, with a wedge shape (arrow).
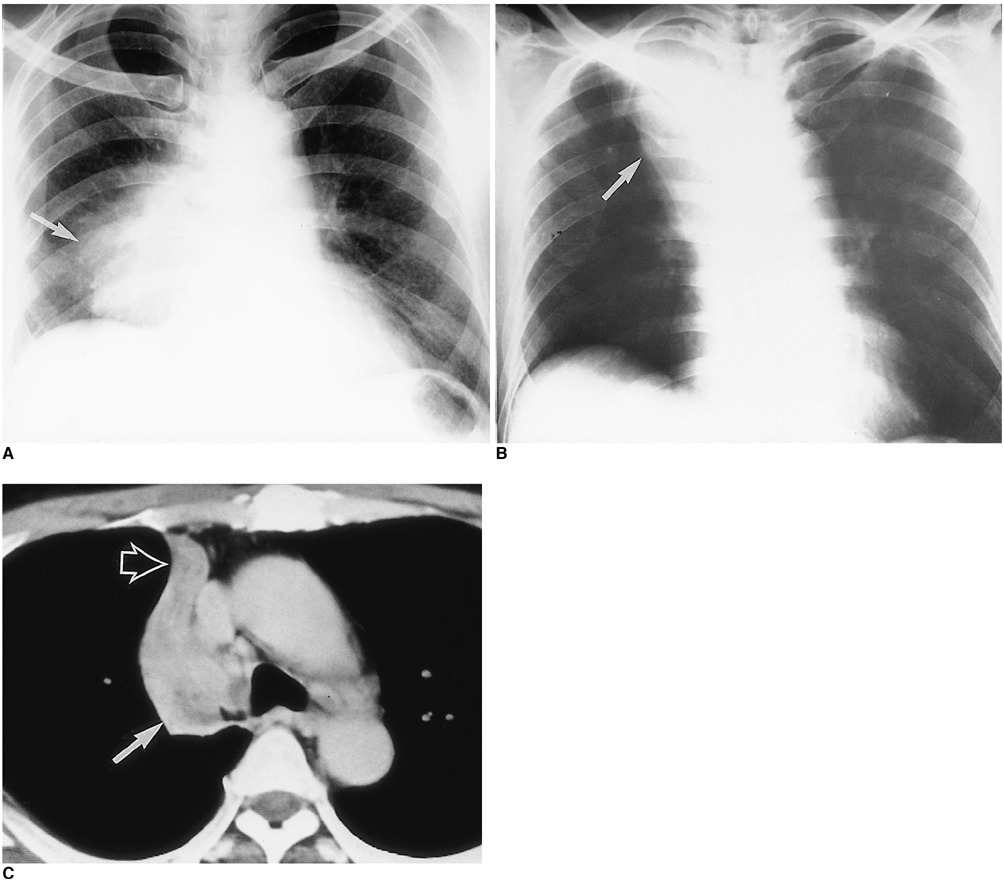
Fig. 2 Migrating right upper lobar atelectasis caused by central lung cancer in a 63-year-old male. A. Erect posteroanterior chest radiograph shows large opacity in right lower lung zone obscuring the right heart border (arrow). B. Supine anteroposterior radiograph obtained three days after (A) shows migration of the atelectatic lobe, with a wedge shape (arrow). C. CT scan obtained at the level of the tracheal carina on the same day as (B) demonstrates a central mass involving the right upper lobar bronchus (solid arrow), resulting in atelectasis of the right upper lobe (open arrow).
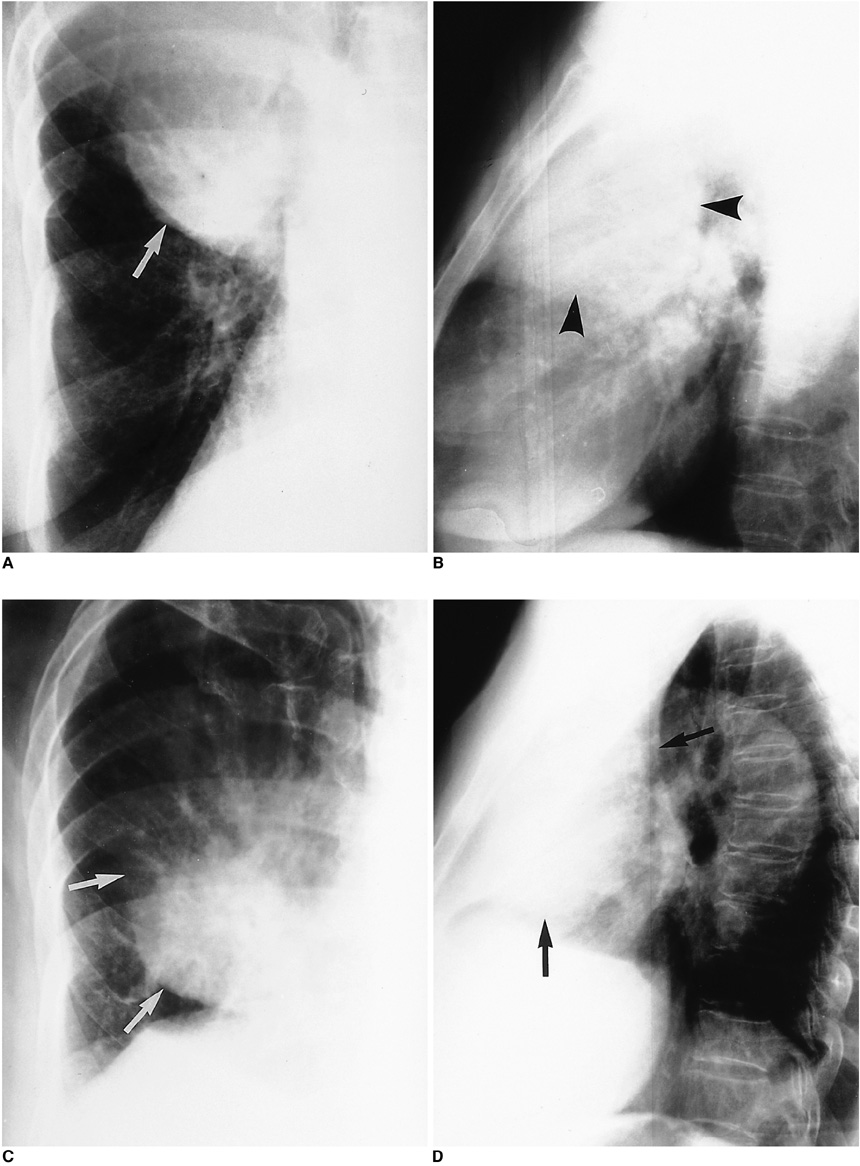
Fig. 3 Migration of combined right upper and middle lobes atelectasis caused by central lung cancer in an 87-year-old female. A. Spot radiograph obtained in supine position during fluoroscopy shows opacity in right upper and middle lung zone obliterating the right cardiac margin (arrow), suggestive of combined atelectasis of the right upper and middle lobes. B. Supine cross-table lateral radiograph shows a large opacity occupying the anterosuperior portion (arrowheads). C. Spot radiograph obtained in erect position during fluoroscopy just after (A) shows the descent of heavy atelectatic lobes to the right lower lung zone (arrows). D. Subsequent erect lateral radiograph shows that the opacity has changed its position, now occupying the anteroinferior portion of the right hemithorax (arrows).
Reference
-
1. Heitzman ER. The lung: Radiologic-pathologic correlation. 1984. 2nd ed. St. Louis: Mosby-Year Book;457–501.2. Lee KS, Logan PM, Primack SL, Muller NL. Combined lobar atelectasis of the right lung: imaging findings. AJR. 1994. 163:43–47.3. Lee KS, Ahn JM, Im J-G, Muller NL. Lobar atelectasis: typical and atypical radiographic and CT findings. Postgrad Radiol. 1995. 15:203–217.4. Felson B. Lung torsion: radiographic findings in nine cases. Radiology. 1987. 162:631–638.5. Graham RJ, Heyd RL, Raval VA, Barrett TF. Lung torsion after percutaneous needle biopsy of lung. AJR. 1992. 159:35–37.6. Meisell R. Case of the spring season: right upper lobe collapse with lobar torsion. Semin Roentgenol. 1980. 15:115–116.7. Huang T-Y, Cho S-R. Torsion of the lung without trauma. Radiology. 1979. 132:25–26.8. Moser ES Jr, Proto AV. Lung torsion: case report and literature review. Radiology. 1987. 162:639–643.9. Berkmen YM, Yankelevitz D, Davis SD, Zanzonico P. Torsion of the upper lobe in pneumothorax. Radiology. 1989. 173:447–449.10. Pinstein ML, Winer-Muram H, Eastridge C, Scott R. Middle lobe torsion following right upper lobectomy. Radiology. 1985. 155:580.11. Munk PL, Vellet AD, Zwirewich C. Torsion of the upper lobe of the lung after surgery: findings on pulmonary angiography. AJR. 1991. 157:471–472.12. Ransdell HT Jr, Ellison RG. Volvulus of a lobe of the lung as a complication of diaphragmatic hernia: a case report. J Thorac Surg. 1953. 25:341–345.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Lobar Atelectasis: Typical and Atypical Radiographic and CT Findings
- Lobar Bronchial Rupture with Persistent Atelectasis after Blunt Trauma
- Clinical characteristics and associated factors of Mycoplasma pneumoniae pneumonia with atelectasis in children
- Correlation of plain film and computed tomography findings of lobar atelectasis
- Atelectasis of Right upper Lobe after Left Thoracotomy under General Inhalation Anesthesia
