Yonsei Med J.
2013 Jan;54(1):209-214. 10.3349/ymj.2013.54.1.209.
Incidence of Venous Air Embolism during Myomectomy: The Effect of Patient Position
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul, Korea. kkj6063@yuhs.ac
- 2Department of Obstetrics and Gynecology, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 1776940
- DOI: http://doi.org/10.3349/ymj.2013.54.1.209
Abstract
- PURPOSE
Venous air embolism (VAE) is characterized by the entrainment of air or exogenous gases from broken venous vasculature into the central venous system. No study exists regarding the effect of patient positioning on the incidence of VAE during abdominal myomectomy. The purpose of this study was to assess the incidence and grade of VAE during abdominal myomectomy in the supine position in comparison to those in the head-up tilt position using transesophageal echocardiography.
MATERIALS AND METHODS
In this study, 84 female patients of American Society of Anesthesiologist physical status I or II who were scheduled for myomectomy under general anesthesia were included. Patients were randomly divided into two groups: supine group and head-up tilt group. Transesophageal echocardiography images were videotaped throughout the surgery. The tapes were then reviewed for VAE grading.
RESULTS
In the supine group, 10% of the patients showed no VAE. Moreover, 10% of the patients were classified as grade I VAE, while 50% were categorized as grade II, 22.5% as grade III, and 7.5% as grade IV. In the head-up tilt group, no VAE was detected in 43.2% of the patients. In addition, 18.2% of the patients were classified as grade I VAE, 31.8% as grade II, and 6.8% as grade III; no patients showed grade IV. VAE grade in the head-up tilt group was significantly lower than that in the supine group (p<0.001).
CONCLUSION
The incidence and grade of VAE in the head-up tilt group were significantly lower than those in the supine group during abdominal myomectomy.
Keyword
MeSH Terms
Figure
-
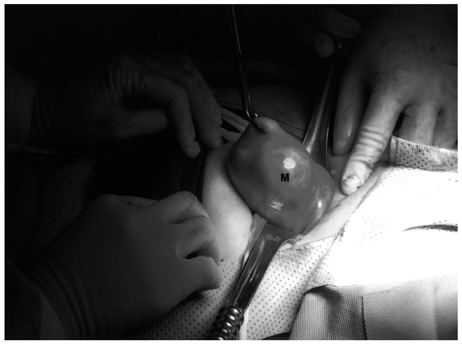
Fig. 1 Externalization of the uterus for excision of a mass of myoma. M, mass of myoma.

Fig. 2 Flow diagram.
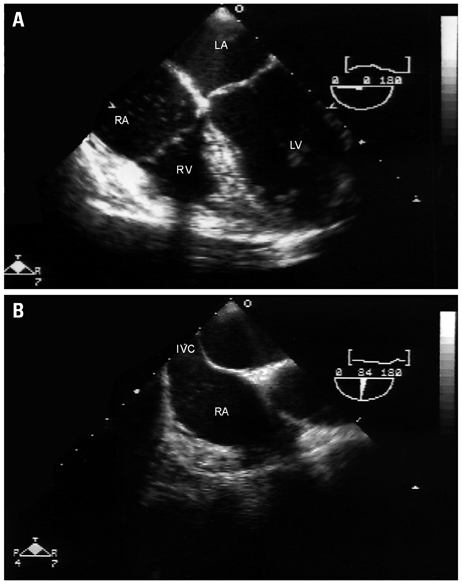
Fig. 3 Venous air emboli detected by transesophageal echocardiography during myomectomy. (A) Mid-esophageal four-chamber view. (B) Bicaval view. RA, right atrium; RV, right ventricle; LA, left atrium; LV, left ventricle; IVC, inferior vena cava.
Reference
-
1. Mommerot A, Perrault LP. Carbon dioxide embolism induced by endoscopic saphenous vein harvesting during coronary artery bypass grafting. J Thorac Cardiovasc Surg. 2006. 132:1502.
Article2. Park EY, Kwon JY, Kim KJ. Carbon dioxide embolism during laparoscopic surgery. Yonsei Med J. 2012. 53:459–466.
Article3. Kama NA. Influence of nitrous oxide anesthesia on venous gas embolism with carbon dioxide and helium during pneumoperitoneum. Surg Endosc. 2001. 15:1237–1238.
Article4. Cottin V, Viale JP, Bouffard Y, Delafosse B. Severe nitrous oxide embolism during venous stripping. Intensive Care Med. 1997. 23:1287–1288.
Article5. Boussuges A, Blanc F, Carturan D. Hemodynamic changes induced by recreational scuba diving. Chest. 2006. 129:1337–1343.
Article6. Risberg J, Englund M, Aanderud L, Eftedal O, Flook V, Thorsen E. Venous gas embolism in chamber attendants after hyperbaric exposure. Undersea Hyperb Med. 2004. 31:417–429.7. Mitchell SJ, Benson M, Vadlamudi L, Miller P. Cerebral arterial gas embolism by helium: an unusual case successfully treated with hyperbaric oxygen and lidocaine. Ann Emerg Med. 2000. 35:300–303.
Article8. Kim CS, Liu J, Kwon JY, Shin SK, Kim KJ. Venous air embolism during surgery, especially cesarean delivery. J Korean Med Sci. 2008. 23:753–761.
Article9. Papadopoulos G, Kuhly P, Brock M, Rudolph KH, Link J, Eyrich K. Venous and paradoxical air embolism in the sitting position. A prospective study with transoesophageal echocardiography. Acta Neurochir (Wien). 1994. 126:140–143.
Article10. Albin MS, Carroll RG, Maroon JC. Clinical considerations concerning detection of venous air embolism. Neurosurgery. 1978. 3:380–384.
Article11. Maroon JC, Goodman JM, Horner TG, Campbell RL. Detection of minute venous air emboli with ultrasound. Surg Gynecol Obstet. 1968. 127:1236–1238.12. Lang S. Precordial Doppler diagnosis of haemodynamically compromising air embolism during caesarean section. Can J Anaesth. 1991. 38:255–256.
Article13. Vacanti CA, Lodhia KL. Fatal massive air embolism during transurethral resection of the prostate. Anesthesiology. 1991. 74:186–187.
Article14. Fong J, Gadalla F, Druzin M. Venous emboli occurring caesarean section: the effect of patient position. Can J Anaesth. 1991. 38:191–195.
Article15. Karuparthy VR, Downing JW, Husain FJ, Knape KG, Blanchard J, Solomon D, et al. Incidence of venous air embolism during cesarean section is unchanged by the use of a 5 to 10 degree head-up tilt. Anesth Analg. 1989. 69:620–623.16. Derouin M, Couture P, Boudreault D, Girard D, Gravel D. Detection of gas embolism by transesophageal echocardiography during laparoscopic cholecystectomy. Anesth Analg. 1996. 82:119–124.
Article17. Kim CS, Kim JY, Kwon JY, Choi SH, Na S, An J, et al. Venous air embolism during total laparoscopic hysterectomy: comparison to total abdominal hysterectomy. Anesthesiology. 2009. 111:50–54.18. Schmandra TC, Mierdl S, Bauer H, Gutt C, Hanisch E. Transoesophageal echocardiography shows high risk of gas embolism during laparoscopic hepatic resection under carbon dioxide pneumoperitoneum. Br J Surg. 2002. 89:870–876.
Article19. Seinera P, Arisio R, Decko A, Farina C, Crana F. Laparoscopic myomectomy: indications, surgical technique and complications. Hum Reprod. 1997. 12:1927–1930.
Article20. Davies A, Hart R, Magos AL. The excision of uterine fibroids by vaginal myomectomy: a prospective study. Fertil Steril. 1999. 71:961–964.
Article21. Spies JB, Cooper JM, Worthington-Kirsch R, Lipman JC, Mills BB, Benenati JF. Outcome of uterine embolization and hysterectomy for leiomyomas: results of a multicenter study. Am J Obstet Gynecol. 2004. 191:22–31.
Article22. Hindley J, Gedroyc WM, Regan L, Stewart E, Tempany C, Hynyen K, et al. MRI guidance of focused ultrasound therapy of uterine fibroids: early results. AJR Am J Roentgenol. 2004. 183:1713–1719.
Article23. Gavai M, Berkes E, Lazar L, Fekete T, Takacs ZF, Urbancsek J, et al. Factors affecting reproductive outcome following abdominal myomectomy. J Assist Reprod Genet. 2007. 24:525–531.
Article24. Balki M, Manninen PH, McGuire GP, El-Beheiry H, Bernstein M. Venous air embolism during awake craniotomy in a supine patient. Can J Anaesth. 2003. 50:835–838.
Article25. Suarez S, Ornaque I, Fábregas N, Valero R, Carrero E. Venous air embolism during Parkinson surgery in patients with spontaneous ventilation. Anesth Analg. 1999. 88:793–794.
Article26. Souders JE. Pulmonary air embolism. J Clin Monit Comput. 2000. 16:375–383.27. Furuya H, Suzuki T, Okumura F, Kishi Y, Uefuji T. Detection of air embolism by transesophageal echocardiography. Anesthesiology. 1983. 58:124–129.
Article28. Gildenberg PL, O'Brien RP, Britt WJ, Frost EA. The efficacy of Doppler monitoring for the detection of venous air embolism. J Neurosurg. 1981. 54:75–78.
Article29. Koo BN, Kil HK, Choi JS, Kim JY, Chun DH, Hong YW. Hepatic resection by the Cavitron Ultrasonic Surgical Aspirator increases the incidence and severity of venous air embolism. Anesth Analg. 2005. 101:966–970.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Venous air embolism during hepatic resection in a patient with liver cirrhosis: A case report
- Cerebral Air Embolism after Removal of Subclavian Venous Catheter: A case report
- Air embolism during anesthesia in the beach chair position for shoulder surgery: A case report
- Fatal Venous Air Embolism during Lung Surgery
- Cerebral Air Embolism after Central Venous Catheter Removal in a Patient with a Patent Foramen Ovale: A Case Report and Literature Review
