Yonsei Med J.
2013 Jan;54(1):166-171. 10.3349/ymj.2013.54.1.166.
The Frequency of Reexpansion Pulmonary Edema after Trocar and Hemostat Assisted Thoracostomy in Patients with Spontaneous Pneumothorax
- Affiliations
-
- 1Department of Emergency Medicine, Wonju College of Medicine, Yonsei University, Wonju, Korea. khyun@yonsei.ac.kr
- 2Department of Emergency Medicine, Andong Hospital, Andong, Korea.
- 3Department of Radiology, Wonju College of Medicine, Yonsei University, Wonju, Korea.
- 4Department of Emergency Medicine, Stony Brook University Hospital, Stony Brook, NY, USA.
- KMID: 1776933
- DOI: http://doi.org/10.3349/ymj.2013.54.1.166
Abstract
- PURPOSE
Several risk factors for development of reexpansion pulmonary edema (REPE) after drainage of pneumothoraces have been reported, but the association between the method of thoracostomy and the development of REPE is unknown. The aim of this study was to compare the frequency of REPE after treatment of spontaneous pneumothorax with trocar or hemostat assisted closed thoracostomy.
MATERIALS AND METHODS
We performed a prospective, observational study including 173 patients with spontaneous pneumothorax who visited the emergency department from January 2007 to December 2008. In 2007, patients were treated with hemostat-assisted drainage, whereas patients in 2008 were treated with trocar-assisted drainage. The main outcome was the development of REPE, determined by computed tomography of the chest 8 hours after closed thoracostomy. Outcomes in both groups were compared using univariate and multivariate analyses.
RESULTS
Ninety-two patients were included, 48 (42 males) of which underwent hemostat-assisted drainage and 44 (41 males) underwent trocar-assisted drainage. The groups were similar in mean age (24+/-10 vs. 26+/-14 respectively). The frequencies of REPE after hemostat- and trocar-assisted drainage were 63% (30 patients) and 86% (38 patients) respectively (p=0.009). In multivariate analysis, trocar-assisted drainage was the major contributing factor for developing REPE (odds ratio=5.7, 95% confidence interval, 1.5-21). Age, gender, size of pneumothorax, symptom duration and laboratory results were similar between the groups.
CONCLUSION
Closed thoracostomy using a trocar is associated with an increased risk of REPE compared with hemostat-assisted drainage in patients with spontaneous pneumothorax.
Keyword
MeSH Terms
Figure
-
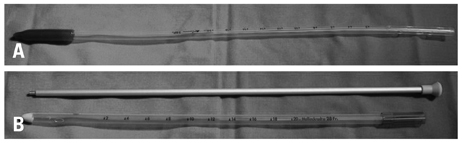
Fig. 1 Traditional thoracostomy tube (A) and trocar tube (B).
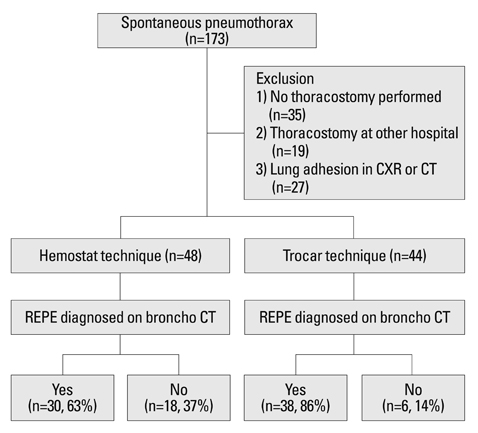
Fig. 2 Study patient flow. CXR, chest X-ray; CT, computed tomography; REPE, reexpansion pulmonary edema.
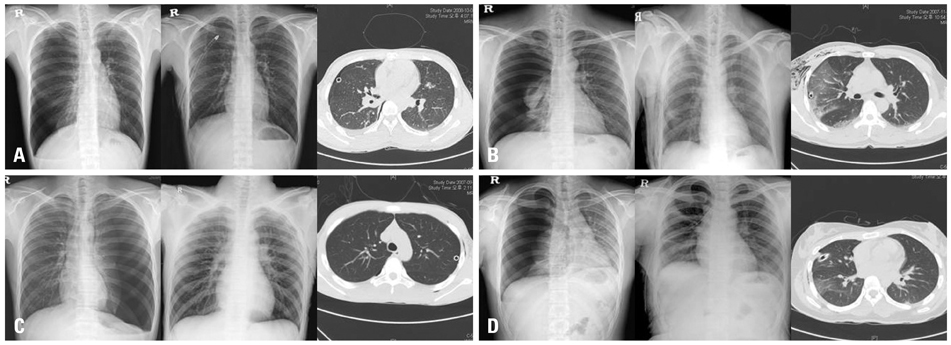
Fig. 3 Reexpansion pulmonary edema (REPE) after thoracostomy. No REPE (A) and REPE (B) after trocar technique. No REPE (C) and REPE (D) after hemostat technique.
Reference
-
1. Carlson RI, Classen KL, Gollan F, Gobbel WG Jr, Sherman DE, Christensen RO. Pulmonary edema following the rapid reexpansion of a totally collapsed lung due to a pneumothorax: a clinical and experimental study. Surg Forum. 1958. 9:367–371.2. Sohara Y. Reexpansion pulmonary edema. Ann Thorac Cardiovasc Surg. 2008. 14:205–209.3. Rozenman J, Yellin A, Simansky DA, Shiner RJ. Re-expansion pulmonary oedema following spontaneous pneumothorax. Respir Med. 1996. 90:235–238.
Article4. Matsuura Y, Nomimura T, Murakami H, Matsushima T, Kakehashi M, Kajihara H. Clinical analysis of reexpansion pulmonary edema. Chest. 1991. 100:1562–1566.
Article5. Kim YK, Kim H, Lee CC, Choi HJ, Lee KH, Hwang SO, et al. New classification and clinical characteristics of reexpansion pulmonary edema after treatment of spontaneous pneumothorax. Am J Emerg Med. 2009. 27:961–967.
Article6. Rhea JT, DeLuca SA, Greene RE. Determining the size of pneumothorax in the upright patient. Radiology. 1982. 144:733–736.
Article7. Collins CD, Lopez A, Mathie A, Wood V, Jackson JE, Roddie ME. Quantification of pneumothorax size on chest radiographs using interpleural distances: regression analysis based on volume measurements from helical CT. AJR Am J Roentgenol. 1995. 165:1127–1130.
Article8. Mahfood S, Hix WR, Aaron BL, Blaes P, Watson DC. Reexpansion pulmonary edema. Ann Thorac Surg. 1988. 45:340–345.
Article9. Choi BG, Park SH, Yun EH, Chae KO, Shinn KS. Pneumothorax size: correlation of supine anteroposterior with erect posteroanterior chest radiographs. Radiology. 1998. 209:567–569.
Article10. Miller WC, Toon R, Palat H, Lacroix J. Experimental pulmonary edema following re-expansion of pneumothorax. Am Rev Respir Dis. 1973. 108:654–656.11. Pavlin J, Cheney FW Jr. Unilateral pulmonary edema in rabbits after reexpansion of collapsed lung. J Appl Physiol. 1979. 46:31–35.
Article12. Sivrikoz MC, Tunçözgür B, Cekmen M, Bakir K, Meram I, Koçer E, et al. The role of tissue reperfusion in the reexpansion injury of the lungs. Eur J Cardiothorac Surg. 2002. 22:721–727.
Article13. Saito S, Ogawa J, Minamiya Y. Pulmonary reexpansion causes xanthine oxidase-induced apoptosis in rat lung. Am J Physiol Lung Cell Mol Physiol. 2005. 289:L400–L406.
Article14. Sautter RD, Dreher WH, MacIndoe JH, Myers WO, Magnin GE. Fatal pulmonary edema and pneumonitis after reexpansion of chronic pneumothorax. Chest. 1971. 60:399–401.
Article15. Tan HC, Mak KH, Johan A, Wang YT, Poh SC. Cardiac output increases prior to development of pulmonary edema after re-expansion of spontaneous pneumothorax. Respir Med. 2002. 96:461–465.
Article16. Kernodle DS, DiRaimondo CR, Fulkerson WJ. Reexpansion pulmonary edema after pneumothorax. South Med J. 1984. 77:318–322.
Article17. Zehtabchi S, Rios CL. Management of emergency department patients with primary spontaneous pneumothorax: needle aspiration or tube thoracostomy? Ann Emerg Med. 2008. 51:91–100. 100.e1
Article18. Hassani B, Foote J, Borgundvaag B. Outpatient management of primary spontaneous pneumothorax in the emergency department of a community hospital using a small-bore catheter and a Heimlich valve. Acad Emerg Med. 2009. 16:513–518.
Article19. Wakai A, O'Sullivan RG, McCabe G. Simple aspiration versus intercostal tube drainage for primary spontaneous pneumothorax in adults. Cochrane Database Syst Rev. 2007. CD004479.
Article20. Hoi K, Turchin B, Kelly AM. How accurate is the Light index for estimating pneumothorax size? Australas Radiol. 2007. 51:196–198.
Article21. Cai W, Lee EY, Vij A, Mahmood SA, Yoshida H. MDCT for computerized volumetry of pneumothoraces in pediatric patients. Acad Radiol. 2011. 18:315–323.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reexpansion Pulmonary Edema Following the Early Decompression of Pneumothorax Occurred after Anesthetic Induction in a Patient with Lung Bulla: A Case Report
- Delayed Onset Contralateral Reexpansion Pulmonary Edema after Tension Pneumothorax: A Case Report
- Reexpansion Pulmonary Edema during Decortication Operation under General Anesthesia - A case report
- Unexpected pulmonary edema and cardiac arrest following wedge resection of spontaneous pneumothorax -A case report-
- Reexpansion Pulmonary Edema after Initial Treatment of Primary Spontaneous Pneumothorax: Small Bore Catheterization versus Chest Tube Thoracostomy
