Gastric Glomus Tumor Showing Hepatic Hemangioma-like Enhancement Pattern on CT
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul, Korea. shkim@radcom.snu.ac.kr
- KMID: 1775845
- DOI: http://doi.org/10.4166/kjg.2011.57.2.134
Abstract
- No abstract available.
MeSH Terms
Figure
-
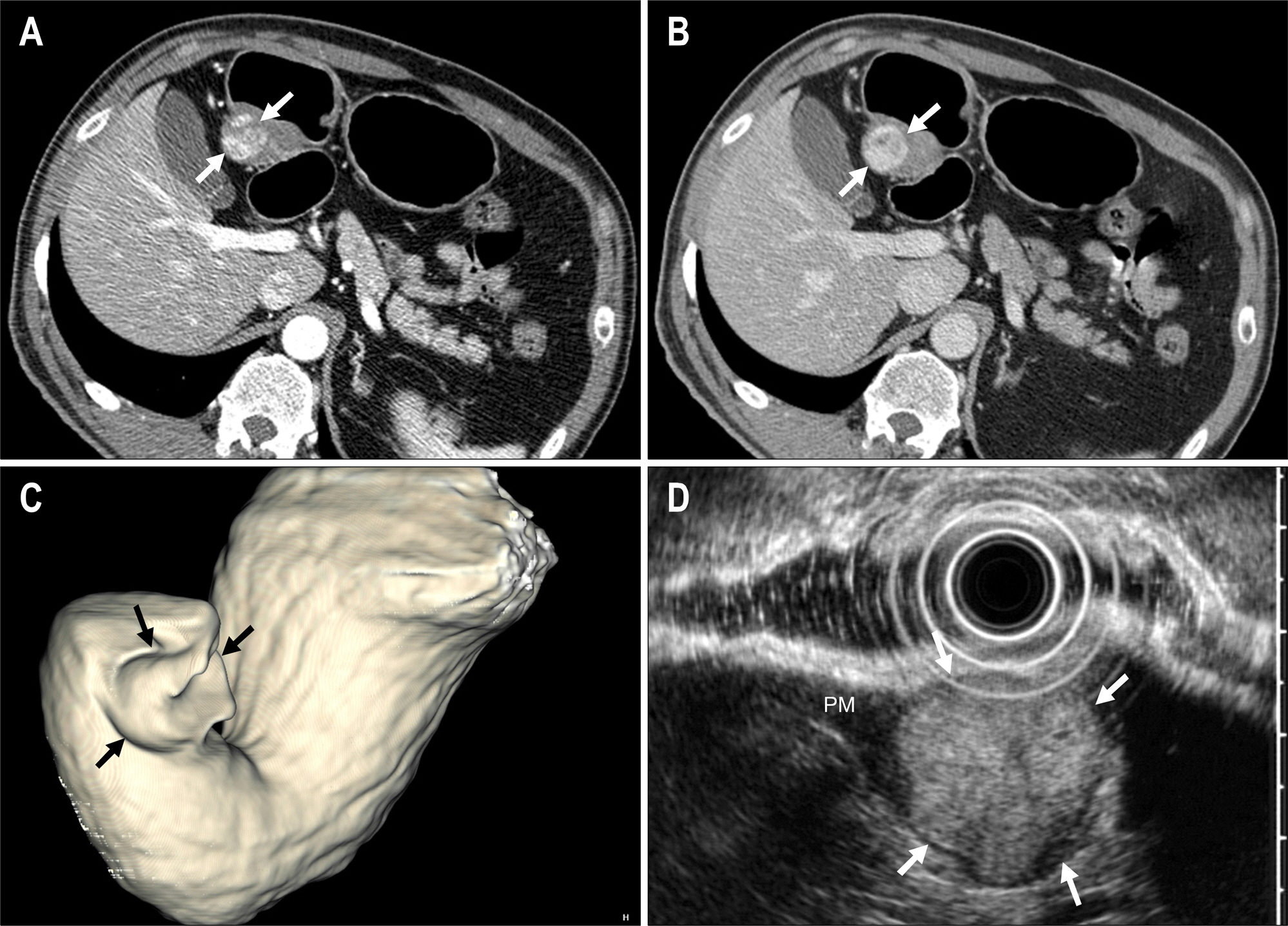
Fig. 1. Dynamic contrast-enhanced CT findings of a gastric glomus tumor. (A) Arterial phase axial CT image showed a 2.4 cm, well-marginated mass (arrows) in the posterior wall of the gastric antrum. Note a peripheral globular and nodular enhancement of the lesion. Overlying gastric mucosa was intact suggesting that this was a subepithelial lesion. Note the thick intact overlying layer measuring 4.1 mm. (B) On portal venous phase CT, the mass (arrows) showed a central fill-in pattern of enhancement like in hepatic hemangioma. Note a very strong degree of enhancement of the lesion. In this patient, lesion-to-aorta enhancement ratio was 0.95. (C) On a 3D surface-rendered CT image, there was a well-demarcated subepithelial mass (arrows) in the posterior wall of the stomach.(D) Endoscopic ultrasonography using a 12 MHz transducer demonstrated a homogeneous echogenic mass (arrows) in the 4 th proper muscle layer (PM). Considering all imaging findings, the tentative radiologic diagnosis was a gastrointestinal stromal tumor.
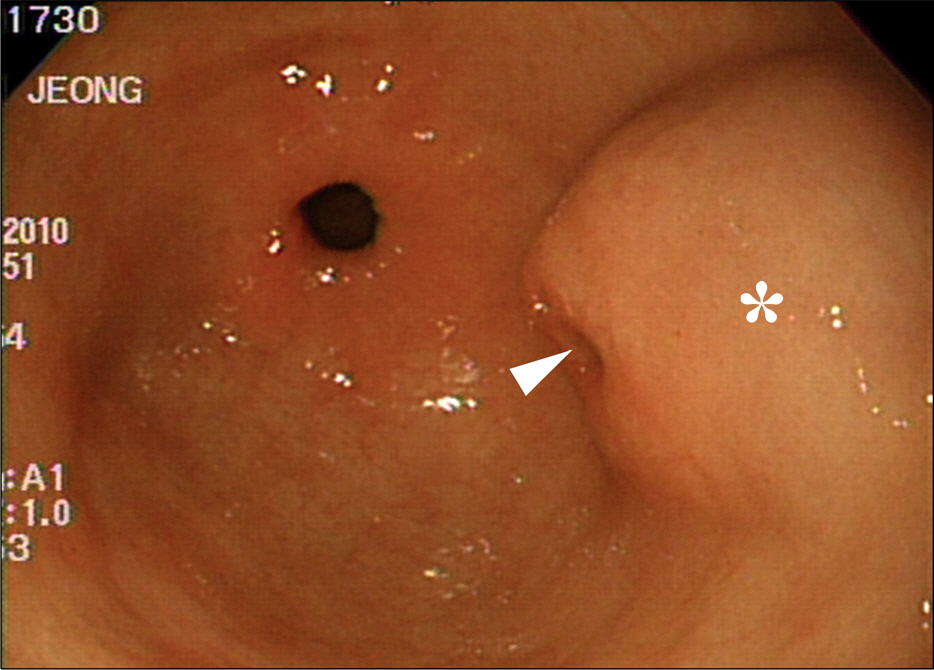
Fig. 2. Gastroscopic finding. Subsequent gastroscopy depicted an intraluminal protruding mass (*) with intact overlying mucosa, confirming this mass was a subepithelial tumor. Note a small ulceration (arrowhead) at the center of the mass.

Fig. 3. Pathologic findings of resected specimen. (A) A photograph of gross specimen obtained after wedge resection demonstrated a 2.4 cm subepithelial tumor (arrows) located in the 4th proper muscle layer of the stomach (PM). (B) A microphotograph showed solid sheets of round, uniform glomus cells surrounding capillaries of varying shape (H&E, ×100). (C) Immunohistochemical staining for synaptophysin was strong positive for glomus tumor.
Reference
-
References
1. Miettinen M, Paal E, Lasota J, Sobin LH. Gastrointestinal glomus tumors: a clinicopathologic, immunohistochemical, and molecular genetic study of 32 cases. Am J Surg Pathol. 2002; 26:301–311.2. Kanwar YS, Manaligod JR. Glomus tumor of the stomach. An ultrastructural study. Arch Pathol. 1975; 99:392–397.3. Lee HW, Lee JJ, Yang DH, Lee BH. A clinicopathologic study of glomus tumor of the stomach. J Clin Gastroenterol. 2006; 40:717–720.
Article4. Hur BY, Kim SH, Choi JY, et al. Can CT features help differentiate gastroduodenal glomus tumors from other gastric submucosal lesions? KCR. 2010. 2010 Oct 18–20;Seoul, Korea.5. Park SH, Han JK, Kim TK, et al. Unusual gastric tumors: radio-logic-pathologic correlation. Radiographics. 1999; 19:1435–1446.
Article6. Cha SH, Cho SB, Kim YW, Park CM. Helical CT appearance of glomus tumor of the stomach. Eur Radiol. 2000; 10:671–673.
Article7. Patel TH, Horton KM, Hruban RH, Fishman EK. Glomus tumor of the stomach: depiction by multidetector CT and three-dimensional volume rendering imaging. Case Report Med. 2010; 2010:126095.
Article8. Harig BM, Rosen Y, Dallemand S, Farman J. The radiology cor-ner*: glomus tumor of the stomach. Am J Gastroenterol. 1975; 63:423–428.9. Park JP, Park SC, Park CK. A case of gastric glomus tumor. Korean J Gastroenterol. 2008; 52:310–314.10. Kim JK, Won JH, Cho YK, Kim MW, Joo HJ, Suh JH. Glomus tumor of the stomach: CT findings. Abdom Imaging. 2001; 26:303–305.
Article11. Hu XY, Hu CH, Fang XM, Zhang TH. Glomus tumor of the gastric body: helical CT findings. Chin Med J. 2007; 120:1289–1291.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Gastric Glomus Tumor
- Diffuse Hepatic Hemangiomatosis without Extrahepatic Involvement in an Adult Patient
- A Case of a Gastric Glomus Tumor with a Positive Cushion Sign
- Wedge-shaped Parenc hymal Enhancement Peripheral to the Hepatic Hemangioma: Two-phase Spiral CT Findings
- A Case of a Symplastic Glomus Tumor
