Myocardial Ischemia Caused by Paroxysmal Supraventricular Tachycardia in a Patient with Anomalous Origin of Right Coronary Artery Arising from Left Sinus of Valsalva
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, CHA University, CHA Bundang Medical Center, Seongnam, Korea.
- 2Cardiology Division, Department of Internal Medicine, College of Medicine, CHA University, Gangnam CHA Hospital, Seoul, Korea. yunkyung.cho@gmail.com
- 3Cardiology Division, Department of Internal Medicine, College of Medicine, CHA University, CHA Bundang Medical Center, Seongnam, Korea.
- KMID: 1769649
- DOI: http://doi.org/10.4070/kcj.2013.43.2.123
Abstract
- Anomalous origin of a coronary artery is rare and does not generally lead to myocardial infarction and paroxysmal supraventricular tachycardia (PSVT). We report an uncommon case of anomalous origin of the right coronary artery (RCA) originating from the left sinus of Valsalva with PSVT and myocardial ischemia. A 58-year-old man presented with PSVT. After arrhythmia subsided, electrocardiogram showed ST and T wave abnormalities, and transient cardiac enzymes were found to be elevated. Coronary CT angiography confirmed that there was anomalous origin of the RCA originating from the left sinus of Valsalva and no intracoronary stenotic lesion. He was managed with conservative treatment, having no symptoms on clinical follow-up for 4 years.
Keyword
MeSH Terms
Figure
-

Fig. 1 Variable changes of ECG. A: ECG show paroxysmal supraventricular tachycardia with pulse rate 190. B: ECG show ST elevation in leads V 1-3 and T inversion in leads II, III, aVF and V 4-6. C: electrocardiogram show T wave inversion in leads II, III, aVF and V 3-6. ECG: electrocardiogram.
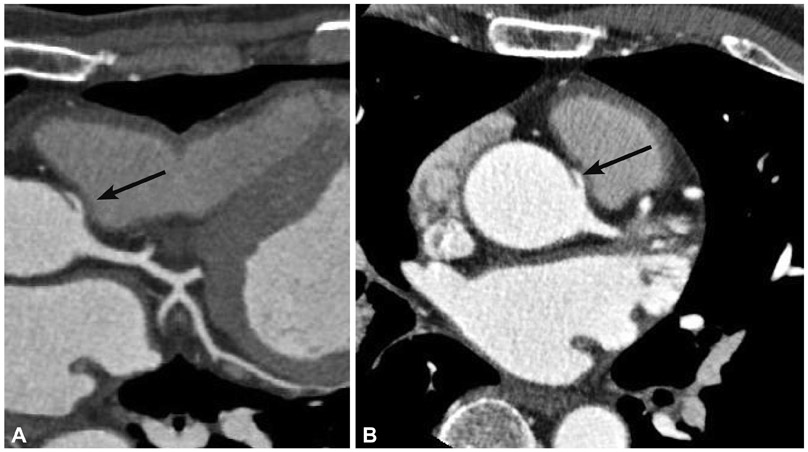
Fig. 2 Anomalous orgin of the right coronary artery with CT coronary angiography. A: multiplanar reformatted image from a multi-detector CT coronary angiogram confirms that the right coronary artery was arising from the left sinus Valsalva with acute angle of the ostium (arrow). B: axial reconstruction anomaly coronary artery takes a course between the right ventricular outflow tract and the aorta (arrow) on axial image.
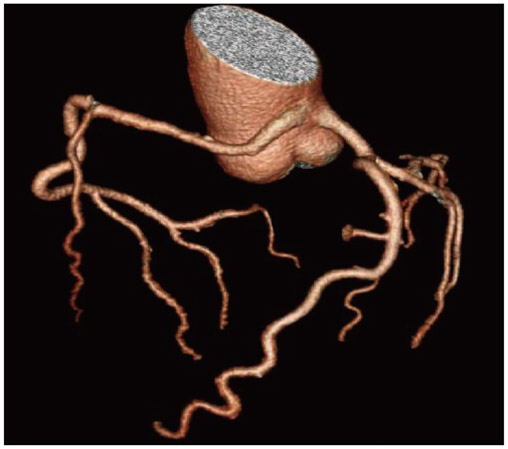
Fig. 3 3D volume rendered multi-detector CT image of the coronary arteries show that there is no stenosis of any coronary artery.
Reference
-
1. Kimbiris D, Iskandrian AS, Segal BL, Bemis CE. Anomalous aortic origin of coronary arteries. Circulation. 1978. 58:606–615.2. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990. 21:28–40.3. Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002. 105:2449–2454.4. Kim JS, Lee JM, Yoon HJ, et al. A case of coronary vessel anomaly of the left circumflex artery originating from the right coronary artery with variant angina. Korean Circ J. 2004. 34:711–714.5. Vincelj J, Todorović N, Marusić P, Puksić S. Anomalous origin of the left coronary artery from the right sinus of Valsalva in a 62-year-old woman with unstable angina pectoris: a case report. Int J Cardiol. 2010. 142:e35–e37.6. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000. 35:1493–1501.7. Dogan SM, Gursurer M, Aydin M, Gocer H, Cabuk M, Dursun A. Myocardial ischemia caused by a coronary anomaly left anterior descending coronary artery arising from right sinus of Valsalva. Int J Cardiol. 2006. 112:e57–e59.8. Lee BY. Anomalous right coronary artery from the left coronary sinus with an interarterial course: is it really dangerous? Korean Circ J. 2009. 39:175–179.9. Park CS, Kim W, Hong SB, Hwang SH, Kim W, An BH. Anomalous origin of the right coronary artery from the main pulmonary artery presenting as angina pectoris in an adult. Korean Circ J. 2008. 38:627–629.10. Tariq R, Kureshi SB, Siddiqui UT, Ahmed R. Congenital anomalies of coronary arteries: diagnosis with 64 slice multidetector CT. Eur J Radiol. 2012. 81:1790–1797.11. Earls JP. Coronary artery anomalies. Tech Vasc Interv Radiol. 2006. 9:210–217.12. Mirchandani S, Phoon CK. Management of anomalous coronary arteries from the contralateral sinus. Int J Cardiol. 2005. 102:383–389.13. Reul RM, Cooley DA, Hallman GL, Reul GJ. Surgical treatment of coronary artery anomalies: report of a 37 1/2-year experience at the Texas Heart Institute. Tex Heart Inst J. 2002. 29:299–307.14. Turer AT, Addo TA, Martin JL, et al. Myocardial ischemia induced by rapid atrial pacing causes troponin T release detectable by a highly sensitive assay: insights from a coronary sinus sampling study. J Am Coll Cardiol. 2011. 57:2398–2405.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sudden Death Associated with Anomalous Left Coronary Artery Origin from Right Sinus of Valsalva with Posterior Course
- An Unusual Pattern of All Three Coronary Arteries Originating from a Single Coronary Artery Arising from the Right Sinus of Valsalva
- A Case of Acute Myocardial Infarction with the Anomalous Origin of the Right Coronary Artery from the Ascending Aorta above the Left Sinus of Valsalva and Left Coronary Artery from the Posterior Sinus of Valsalva
- Anomalous Right Coronary Artery From the Left Coronary Sinus With an Interarterial Course: Is It Really Dangerous?
- Anomalous Origin of the Left Coronary Artery Leading to Myocardial Infarction in a 14-year-old Boy
