Tubular Foreign Body or Stent: Safe Retrieval or Repositioning Using the Coaxial Snare Technique
- Affiliations
-
- 1Department of Radiology, Kyungpook National University School of Medicine, Daegu, Korea. chungjw@radcom.snu.ac.kr
- 2Department of Radiology, Seoul National University College of Medicine, Institute of Radiation Medicine, SNUMRC (Seoul National University Medical Research Center), and Clinical Research Institute, Seoul National University Hospital.
- KMID: 1758444
- DOI: http://doi.org/10.3348/kjr.2002.3.1.30
Abstract
OBJECTIVE
To evaluate the utility and advantages of the coaxial snare technique in the retrieval of tubular foreign bodies.
MATERIALS AND METHODS
Using the coaxial snare technique, we attempted to retrieve tubular foreign bodies present in seven patients. The bodies were either stents which were malpositioned or had migrated from their correct position in the vascular system (n=2), a fragmented venous introducer sheath (n=1), fragmented drainage catheters in the biliary tree (n=2), or fractured external drainage catheters in the urinary tract (n=2). After passing a guidewire and/or a dilator through the lumina of these foreign bodies, we introduced a loop snare over the guidewire or dilator, thus capturing and retrieving them.
RESULTS
In all cases, it was possible to retrieve or reposition the various items, using a minimum-sized introducer sheath or a tract. No folding was involved. In no case were surgical procedures required, and no complications were encountered.
CONCLUSION
The coaxial snare technique, an application of the loop snare technique, is a useful and safe method for the retrieval of tubular foreign bodies, and one which involves minimal injury to the patient.
MeSH Terms
Figure
-
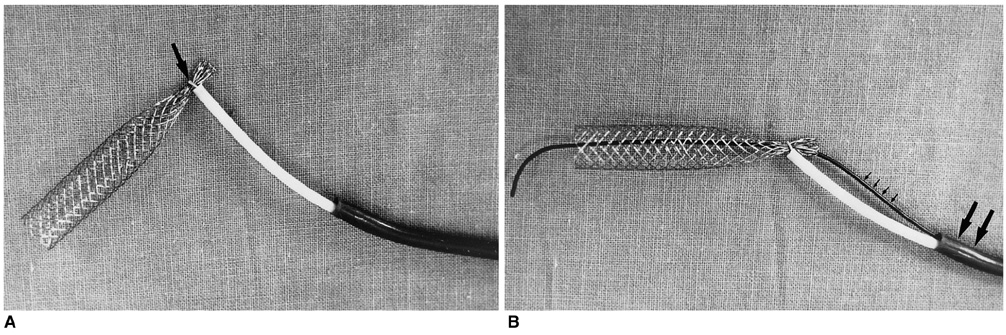
Fig. 1 Ex-vivo study of coaxial snaring of a vascular stent. A. Simple snaring (arrow) of a Niti-S stent results in the formation of a right angle between the stent and the snare axis. Retrieval of the stent in this configuration would therefore be traumatic. B. Coaxial snaring of the stent while a guidewire (small arrows) runs through it reduces the angle between the stent and the introducer sheath (large arrows), thus allowing repositioning of the stent through the TIPS tract.
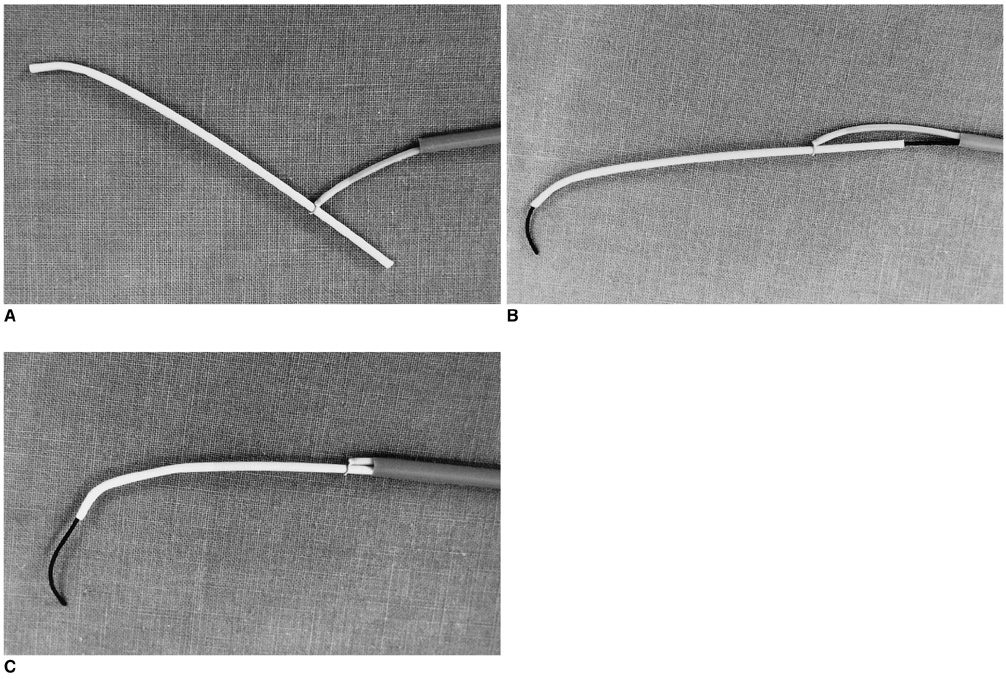
Fig. 2 Ex-vivo study of coaxial snaring of a small-bore catheter fragment (5-F). A. Simple snaring of the catheter fragment also causes an angulation problem. B. Coaxial snaring reduces the angle between the catheter fragment and the snaring catheter. Note that the guidewire was positioned through the lumen of the catheter fragment. C. There is smooth engagement between the catheter fragment and the 10-F sheath.

Fig. 3 Ex-vivo study of the retrieval of a large-bore sheath fragment (8-F internal diameter and 10-F outer diameter) using a modified coaxial snare technique. A. In the large-bore fragmented vascular sheath, the simple coaxial snare technique does not allow engagement between the fragment and the 10-F or 12-F introducer sheath. The overall profile of the coaxial retrieval system is more than 14-F, with a shoulder between the 10-F introducer sheath (black arrow) and the sheath fragment (white arrows). B. The loop snare introduced through the smaller sheath (10-F) captures the fractured vascular sheath. Separate access is obtained via the larger sheath (12-F), and the central lumen of the fractured sheath is located with an angiographic catheter and guidewire. C. After engaging a dilator (small black arrow) at its end, the fragmented sheath (white arrow) is seen to be smoothly aligned with the introducer sheath (large black arrow).
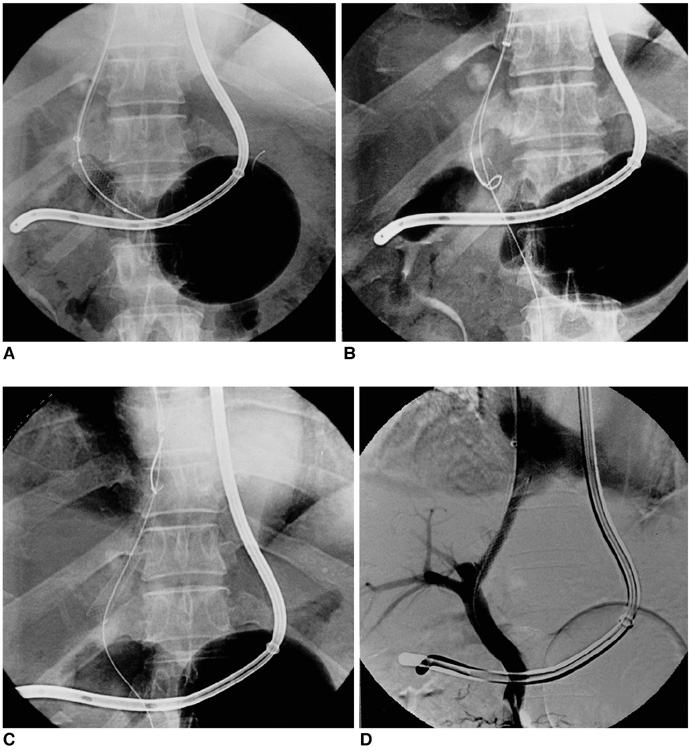
Fig. 4 Relocation of a stent employed in a TIPS procedure using the coaxial snare technique. A. The deployed nitinol stent has migrated caudad to the main portal vein. The inflated gastric balloon signifies that the patient is actively bleeding. B. The loop of an Amplatz gooseneck snare is introduced over the preexisting guidewire and positioned around the stent. C. After a loop snare was used to squeeze the proximal end of the stent, this was pulled back and relocated to its appropriate position. D. A digital subtraction angiogram obtained after relocation shows rapid flow from the superior mesenteric vein to the right atrium via the created TIPS tract.

Fig. 5 Retrieval of a large-bore sheath fragment using a modified coaxial snare technique. A. During bedside placement of an internal jugular venous catheter, the tip of this sheared off and lodged in the right atrium. The fragment was captured by a gooseneck snare and pulled back into the inferior vena cava. B. The femoral vein was punctured a second time, just above the puncture site for the loop snare, and a 12-F vascular sheath was introduced. With the assistance of a loop snare, the fragment has successfully engaged with the dilator of the vascular sheath. C. The whole system was slowly withdrawn until the sheath fragment appeared at the puncture site. The linear mark represents the puncture site for the loop snare.
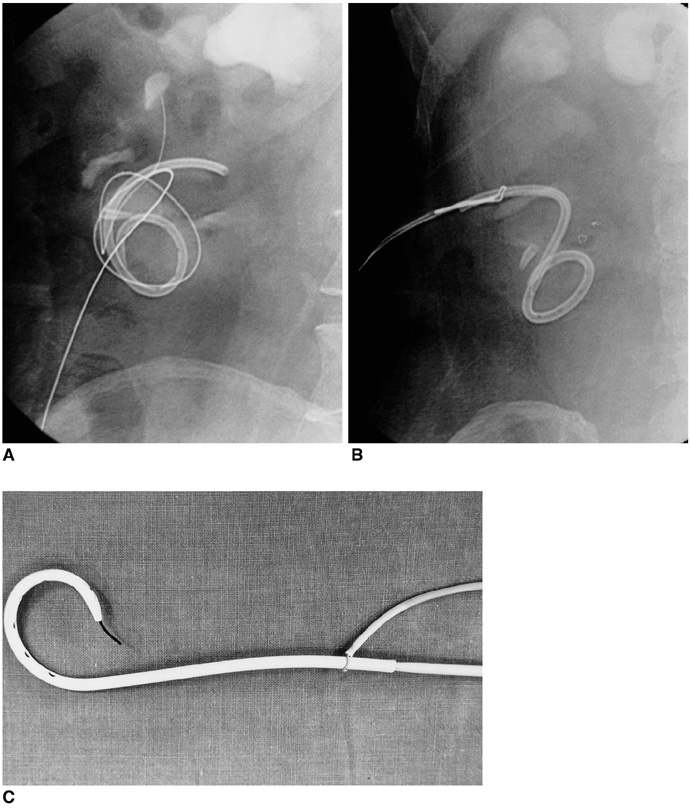
Fig. 6 Retrieval of a catheter fragment (10.2-F) from the renal pelvis using the coaxial snare technique. A. Because the fragmented catheter was tightly attached to the wall of the pelvocalyceal system, other method failed to capture it. B. After passing a guidewire through the catheter lumen, the end of the catheter was easily captured by a loop snare introduced coaxially over the guidewire. A second small fragmented catheter tip is also seen. C. Photograph of the entire extracted retrieval system. The catheter fragment is firmly grasped by the retracting loop snare, and for smooth extraction, a 10-F dilator has been introduced into the catheter fragment over the guidewire.
Cited by 1 articles
-
Percutaneous transhepatic biliary drainage catheter fracture: A case report
Jia Rui Kwan, Keith Sheng Hng Low, Rahul Lohan, Vishal G Shelat
Ann Hepatobiliary Pancreat Surg. 2018;22(3):282-286. doi: 10.14701/ahbps.2018.22.3.282.
Reference
-
1. Dotter CT, Rosch J, Bilbao MC. Transluminal extraction of catheter and guidewire fragments from the heart and great vessels: 29 collected cases. AJR. 1971. 111:467–472.2. Bloomfield DA. The nonsurgical retrieval of intracardiac foreign bodies: an international survey. Cathet Cardiovasc Diagn. 1978. 4:1–14.3. Uflaker R, Lima S, Melichar AC. Intravascular foreign bodies: percutaneous retrieval. Radiology. 1986. 160:731–735.4. Selby JB, Tegtmeyer CJ, Bittner GM. Experience with new retrieval forceps for foreign body removal in the vascular, urinary, and biliary systems. Radiology. 1990. 176:535–538.5. Dondeliger RF, Lepontre B, Kurdziel JC. Percutaneous vascular foreign body retrieval: experience of an 11-year period. Eur J Radiol. 1991. 12:4–10.6. Siegel EL, Robertson EF. Percutaneous transfemoral retrieval of a free-floating titanium Greenfield filter with an Amplatz gooseneck snare. J Vasc Interv Radiol. 1993. 4:565–568.7. Cekirge S, Weiss JP, Foster RG, Neiman HL, McLean GK. Percutaneous retrieval of foreign bodies: experience with the nitinol gooseneck snare. J Vasc Interv Radiol. 1993. 4:805–810.8. Egglin TKP, Dickey KW, Rosenblatt M, Pollak JS. Retrieval of intravascular foreign bodies: experience in 32 cases. AJR. 1995. 164:1259–1264.9. Hartnell GG, Jordan SJ. Percutaneous removal of a misplaced Palmaz stent with a coaxial snare technique. J Vasc Interv Radiol. 1995. 6:799–801.10. Coleman CC, Kimura Y, Castaneda-Zuniga WR. Interventional techniques in the ureter. Semin Intervent Radiol. 1984. 1:24–37.11. LeRoy AJ, Williams HJ Jr, Segura JW, Patterson DE, Benson RC Jr. Indwelling ureteral stents: percutaneous management of complications. Radiology. 1986. 158:219–222.12. Abramson AF, Javit DJ, Mitty HA, Train JS, Dan SJ. Wallstent migration following deployment in right and left bile ducts. J Vasc Interv Radiol. 1992. 3:463–465.13. Johanson JF, Schmalz MJ, Geenen JE. Incidence and risk factors for biliary and pancreatic stent migration. Gastrointest Endosc. 1992. 38:341–346.14. Nemcek AA Jr, Vogelzang RL. Modified use of the tip-deflecting wire in manipulation of foreign bodies. AJR. 1987. 149:777–779.15. Boren SR, Dotter CT, McKinney M, Rosch J. Percutaneous removal of ureteral stents. Radiology. 1984. 152:230–231.16. Park JH, Yoon DY, Han JK, Kim SH, Han MC. Retrieval of intravascular foreign bodies with the snare and catheter capture technique. J Vasc Interv Radiol. 1992. 3:581–582.17. Katske FA, Celis P. Technique for removal of migrated double-J ureteral stent. Urology. 1991. 37:579.18. Savader SJ, Brodkin J, Osterman FA. In-situ formation of a loop snare for retrieval of a foreign body without a free end. Cardiovasc Intervent Radiol. 1996. 19:298–301.19. Millan VG. Retrieval of intravascular foreign bodies using a modified bronchoscopic forceps. Radiology. 1978. 129:587–589.20. Kim SH, Song IS, Kim JH, Park JH, Han MC. Retrieval of a guidewire introducer by catheter-capture from the proximal inferior vena cava: technical note. Cardiovasc Intervent Radiol. 1991. 14:252–253.21. Curry JL. Recovery of detached intravascular catheter or guide wire fragments: a proposed method. AJR. 1969. 105:894–896.22. Fisher RG, Ferreyro R. Evaluation of current techniques for nonsurgical removal of intravascular iatrogenic foreign bodies. AJR. 1978. 130:541–548.23. Fjalling M, List AR. Transvascular retrieval of an accidentally ejected tip occluder and wire. Cardiovasc Intervent Radiol. 1982. 5:34–36.24. Rossi P. Hook catheter technique for transfemoral removal of foreign body from right side of the heart. AJR. 1970. 108:101–106.25. Sanchez RB, Roberts AC, Valji K, Lengle S, Bookstein JJ. Wallstent misplaced during transjugular placement of an intrahepatic portosystemic shunt: retrieval with a loop snare. AJR. 1992. 159:129–130.26. Cekirge S, Foster RG, Weiss JP, McLean GK. Percutaneous removal of an embolized Wallstent during a transjugular intrahepatic portosystemic shunt procedure. J Vasc Interv Radiol. 1993. 4:559–560.27. Cohen GS, Ball DS. Delayed wallstent migration after a transjugular intrahepatic portosystemic shunt procedure: relocation with a loop snare. J Vasc Interv Radiol. 1993. 4:561–563.28. Foster-Smith KW, Garratt KN, Higano ST, Holmes DR. Retrieval techniques for managing flexible intracoronary stent misplacement. Cathet Cardiovasc Diagn. 1985. 11:623–628.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Percutaneous Transluminal Retrieval of Catheter Foreign Body Using Loop-Snare Technique
- Percutaneous Retrieval of a Migrated Surgical Drainage Tube in the Chest Wall with the Nitinol Goose Neck Snare
- Non-surgical retrieval of foreign bodies
- Foreign Body Removal by Snare Loop: During Intracranial Stent Procedure
- Percutaneous Retrieval of an Intravascular Catheter Embolus
