J Korean Med Sci.
2004 Apr;19(2):291-293. 10.3346/jkms.2004.19.2.291.
Pacemaker Lead Endocarditis Caused by Achromobacter xylosoxidans
- Affiliations
-
- 1Divisions of Cardiology and Infectious Disease, Chonnam National University Hospital, Gwangju, Korea. chojg@unitel.co.kr
- 2Division of Cardiology, Wonkwang University Hospital, Iksan, Korea.
- KMID: 1733492
- DOI: http://doi.org/10.3346/jkms.2004.19.2.291
Abstract
- We report the case of a 35-yr-old patient who presented with high fever and chills. He had undergone a patch closure of the ventricular septal defect 18 yr before. One year later, a VVI pacemaker was implanted via the right subclavian vein because of complete heart block. Nine years after that, a new VVI pacemaker with another right ventricular electrode was inserted controlaterally and the old pacing lead was abandoned. Trans-thoracic and trans-esophageal echocardiogram identified the pacemaker lead in the right ventricle (RV) attaching hyperechoic materials and also a fluttering round hyperechoic mass with a stalk in the RV outflow tract. Cultures in blood and pus from pacemaker lead grew Achromobacter xylosoxidans. A diagnosis of pacemaker lead endocarditis due to Achromobacter xylosoxidans was made. In this regards, the best treatment is an immediate removal of the entire pacing system and antimicrobial therapy.
MeSH Terms
Figure
-
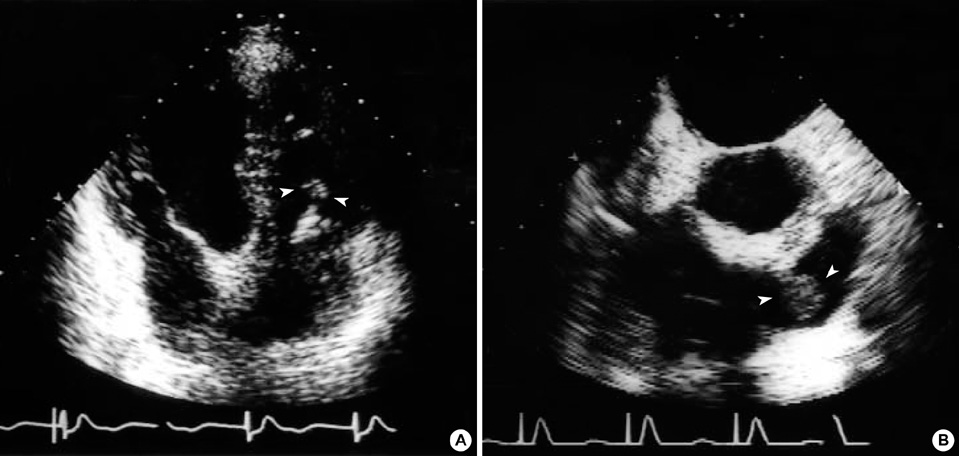
Fig. 1 (A) Transthoracic echocardiogram, apical four-chamber view. A pacemaker lead with attached hyperechoic materials is seen in the right ventricle. (B) Transesophageal echocardiogram. A hyperechoic mass with a stalk is freely movable in the right ventricular outflow tract.

Fig. 2 The removed electrode. It was destroyed and attached with yellow-brown friable materials.
Reference
-
1. Klug D, Lacroix D, Savoye C, Goullard L, Grandmougin D, Hennequin JL, Kacet S, Lekieffre J. Systemic infection related to endocarditis on pacemaker leads: clinical presentation and management. Circulation. 1997. 95:2098–2107.2. Banos R, Gomez J, Sanchez B, de la Morena G, Simarro E, Garcia del Real F. Pacemaker lead endocarditis: analysis of 11 cases. Enferm Infecc Microbiol Clin. 2000. 18:267–270.3. Cacoub P, Leprince P, Nataf P, Hausfater P, Dorent R, Wechsler B, Bors V, Pavie A, Piette JC, Gandjbakhch I. Pacemaker infective endocarditis. Am J Cardiol. 1998. 82:480–484.
Article4. Voet JG, Vandekerckhove YR, Muyldermans LL, Missault LH, Matthys LJ. Pacemaker lead infection: report of three cases and review of the literature. Heart. 1999. 81:88–91.
Article5. Victor F, De Place C, Camus C, Le Breton H, Leclercq C, Pavin D, Mabo P, Daubert C. Pacemaker lead infection: echocardiographic features, management, and outcome. Heart. 1999. 81:82–87.
Article6. Miralles A, Moncada V, Chevez H, Rodriguez R, Granados J, Castells E. Pacemaker endocarditis: approach for lead extraction in endocarditis with large vegetations. Ann Thorac Surg. 2001. 72:2130–2132.
Article7. Jacobs JA, Stobberingh EE, Schouten HC. Fatal infection due to Alcaligenes xylosoxidans subsp. Xylosoxidans in a neutropenic host. Clin Microbiol Newslett. 1992. 14:182–184.
Article8. Duggan JM, Goldstein SJ, Chenoweth CE, Kauffman CA, Bradley SF. Achromobacter xylosoxidans bacteremia: report of four cases and review of the literature. Clin Infect Dis. 1996. 23:569–576.
Article9. Sasaki H, Kawai H, Sawamura T, Takiya H. A case report of aortic valve and VSD Dacron patch infective endocarditis after VSD patch closure 15 years ago. Nippon Kyobu Geka Gakkai Zasshi. 1993. 41:1373–1377.10. Dalal A, Asirvatham SJ, Chandrasekaran K, Seward JB, Tajik AJ. Intracardiac echocardiography in the detection of pacemaker lead endocarditis. J Am Soc Echocardiogr. 2002. 15:1027–1028.
Article11. Tan HH, Ling LH, Ng WL, Cheng A. Diagnosis of pacemaker lead infection using transoesophageal echocardiography: a case report. Ann Acad Med Singapore. 2000. 29:97–100.12. Ku GW, Kang SK, Won TH, Kim SW, Yu JH, Na MH, Lim SP, Lee Y. Endocarditis with intracardiac migration of transvenous permanent pacing lead: 1 case report. Korean J Thorac Cardiovasc Surg. 2002. 35:831–834.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Septic Shock caused by Achromobacter xylosoxidans in an Immunocompetent Female Patient after Extracorporeal Shock Wave Lithotripsy for a Ureteral Stone
- A case of scalp abscess caused by Achromobacter xylosoxidans after vacuum delivery
- A Case of Chronic Dacryocystitis Caused by Achromobacter Xylosoxidans
- Continuous Ambulatory Peritoneal Dialysis-Associated Peritonitis Caused by Achromobacter xylosoxidans: A Case Report and Comprehensive Literature Review
- A Case of Peritonitis Due to Achromobacter xylosoxidans subsp. xylosoxidans in a Patient Undergoing Continuous Ambulatory Peritoneal Dialysis (CAPD)
