Chonnam Med J.
2010 Aug;46(2):99-104. 10.4068/cmj.2010.46.2.99.
Changes in the Management of High Grade Renal Injury and the Usefulness of Nonoperative Management
- Affiliations
-
- 1Department of Urology, Chonnam National University Medical School, Gwangju, Korea. drjsi@yahoo.co.kr
- KMID: 1730006
- DOI: http://doi.org/10.4068/cmj.2010.46.2.99
Abstract
- Despite the increasing incidence of renal trauma, the management of major renal injuries remains controversial. We reviewed our experience to identify changes in renal injury management and to clarify the usefulness of nonsurgical management. We retrospectively analyzed the charts and films of 128 patients admitted to our hospital for renal injury from March 2003 to April 2010. We classified the patients into three groups according to treatment methods: conservative treatment, surgical treatment, and percutaneous embolization, and made comparisons between the first (Group A) and last (Group B) 64 patients. Patients were 97 males (75.8%) and 31 females (24.2%) with a mean age of 36.0 years. The main cause of injury was related to traffic accidents in 62 cases (48.4%), and the most common associated injury was hemoperitoneum in 31 cases (24.2%). According to radiologic and operative findings, the cases were classified as follows: grade I in 14 cases (10.9%), grade II in 16 cases (12.5%), grade III in 36 cases (28.1%), grade IV in 48 cases (37.5%), and grade V in 15 cases (11.7%). All patients with low grade (grade I, II) and grade V renal injury were treated with conservative therapy and operation, respectively, and there were no differences between Group A and Group B. Grade III and IV renal injury cases showed some difference in management between the two groups, however. In Group B compared with Group A, all grade III renal injury patients were successfully treated with nonoperative management (p=0.171). The percutaneous embolization rate was increased (Group A: 12.0%, Group B: 21.7%), and the surgical treatment rate was decreased (Group A: 16.0%, Group B: 4.3%) in patients with grade IV renal injuries (p=0.325). Nonoperative management was successfully performed even in patients with grade III and IV renal injury; therefore, it will be considered as the first treatment of choice in most high-grade renal injuries except for grade V renal injuries.
Keyword
MeSH Terms
Figure
-
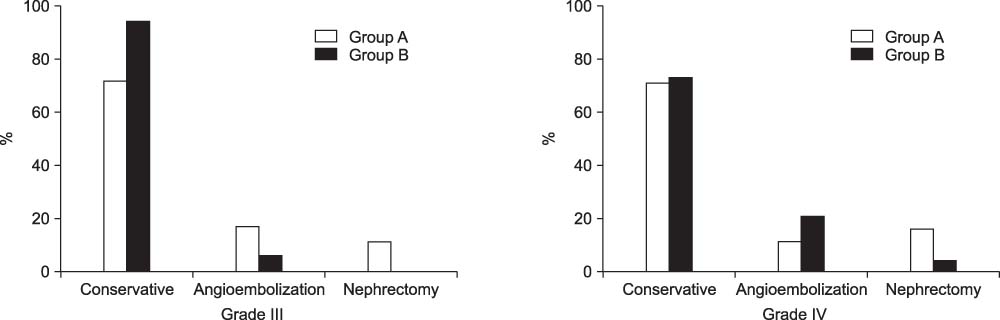
Fig. 1 Comparison of treatment between classification (Grade III, IV) in Group A and Group B (%). *All patients with grade V renal injury were treated with nephrectomy, and it showed no difference between two groups.
Reference
-
1. Nash PA, Carroll PR. Mc-Aninch JW, editor. Staging of renal trauma. Traumatic and reconstructive urology. 1996. 1st ed. Philadelphia: Saunders;95–104.2. Moore EE, Shackford S, Pachter HL, McAninch JW, Browner BD, Champion HR, et al. Organ injury scaling: spleen, liver, and kidney. J Trauma. 1989. 29:1664–1666.3. Guerriero WG. Guerriero WG, Devin CJ, editors. Renal trauma. Urological injuries. 1984. 1st ed. Norwalk: Appleton Century Crofts;9–44.4. Cass AS, Luxenberg M. Conservative or immediate surgical management of blunt renal injuries. J Urol. 1983. 130:11–16.
Article5. Smith EM, Elder JS, Spirnak JP. Major blunt renal trauma in the pediatric population: is a nonoperative approach indicated? J Urol. 1993. 149:546–548.
Article6. Buckley JC, McAninch JW. Selective management of isolated and nonisolated grade IV renal injuries. J Urol. 2006. 176:2498–2502.
Article7. Altman AL, Haas C, Dinchman KH, Spirnak JP. Selective nonoperative management of blunt grade 5 renal injury. J Urol. 2000. 164:27–30.
Article8. Sofocleous CT, Hinrichs C, Hubbi B, Brountzos E, Kaul S, Kannarkat G, et al. Angiographic findings and embolotherapy in renal arterial trauma. Cardiovasc Intervent Radiol. 2005. 28:39–47.
Article9. Lee JY, Cass AS. McAninch JW, editor. Renal injuries in children. Traumatic and reconstructive urology. 1996. 1st ed. Philadelphia: Saunders;127–133.10. Khan AB, Reid AW. Management of renal stab wounds by arteriographic embolisation. Scand J Urol Nephrol. 1994. 28:109–110.11. Beaujeux R, Saussine C, al-Fakir A, Boudjema K, Roy C, Jacqmin D, et al. Superselective endo-vascular treatment of renal vascular lesions. J Urol. 1995. 153:14–17.
Article12. McAninch JW, Carroll PR, Klosterman PW, Dixon CM, Greenblatt MN. Renal reconstruction after injury. J Urol. 1991. 145:932–937.
Article13. Kim HG, Kim SJ, Kim KM, Choi H. Kidney injury in children. Korean J Urol. 1992. 33:1038–1044.14. Boone TB, Gilling PJ, Husmann DA. Ureteropelvic junction disruption following blunt abdominal trauma. J Urol. 1993. 150:33–36.
Article15. Buckley JC, McAninch JW. The diagnosis, management, and outcomes of pediatric renal injuries. Urol Clin North Am. 2006. 33:33–40.
Article16. McAninch JW, Santucci RA. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Renal and ureteral trauma. Campbell-Walsh urology. 2007. 9th ed. Philadelphia: Saunders;1274–1292.17. Wessells H. Evaluation and management of renal trauma in the 21st century. AUA Update Ser. 2002. 21:234–239.18. Mee SL, McAninch JW, Robinson AL, Auerbach PS, Carroll PR. Radiographic assessment of renal trauma: a 10-year prospective study of patient selection. J Urol. 1989. 141:1095–1098.
Article19. Herschorn S, Radomski SB, Shoskes DA, Mahoney J, Hirshberg E, Klotz L. Evaluation and treatment of blunt renal trauma. J Urol. 1991. 146:274–277.
Article20. Eastham JA, Wilson TG, Ahlering TE. Urological evaluation and management of renal proximity stab wounds. J Urol. 1993. 150:1771–1773.21. Bernath AS, Schutte H, Fernandez RR, Addonizio JC. Stab wounds of the kidney: conservative management in flank penetration. J Urol. 1983. 129:468–470.
Article22. Kyoun JK, Cho SY, Lee JB. Renal trauma in abdominal and thoracic stab injury: comparison of incidence and degree of injury according to the stab entrance site. Korean J Urol. 2003. 44:328–333.23. Fisher RG, Ben-Menachem Y, Whigham C. Stab wounds of the renal artery branches: angiographic diagnosis and treatment by embolizatin. AJR Am J Roentgenol. 1989. 152:1231–1235.
Article24. Alsikafi NF, Rosenstein DI. Staging, evaluation, and nonoperative management of renal injuries. Urol Clin North Am. 2006. 33:13–19.
Article25. Peters PC, Bright TC 3rd. Blunt renal injuries. Urol Clin North Am. 1977. 4:17–28.
Article26. Husmann DA, Morris JS. Attempted nonoperative management of blunt renal lacerations extending through the corticomedullary junction: the short-term and long-term sequelae. J Urol. 1990. 143:682–684.
Article27. Moudouni SM, Patard JJ, Manunta A, Guiraud P, Guille F, Lobel B. A conservative approach to major blunt renal lacerations with urinary extravasation and devitalized renal segments. BJU Int. 2001. 87:290–294.
Article28. Danuser H, Wille S, Zöscher G, Studer U. How to treat blunt kidney ruptures: primary open surgery or conservative treatment with deferred surgery when necessary? Eur Urol. 2001. 39:9–14.
Article29. Buckley JC, McAninch JW. Selective management of isolated and nonisolated grade IV renal injuries. J Urol. 2006. 176:2498–2502.
Article30. McAninch JW. Selective nonoperative management of blunt grade 5 renal injury. J Urol. 2000. 164:30–31. (Ed. comment).
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Management of Adult Blunt Renal Injury: A 10-Year Retrospective Review at a Single Institution
- Nonoperative Management Guideline of Liver Injury
- Nonoperative Management of Blunt Abdominal Trauma with Hemoperitoneum
- Successful nonoperative management of a simultaneous high-grade splenic injury and devascularized kidney in Australia: a case report
- Management of High-grade Blunt Renal Trauma
