Yonsei Med J.
2005 Aug;46(4):546-554. 10.3349/ymj.2005.46.4.546.
Biomechanical Assessment with Electromyography of Post-Stroke Ankle Plantar Flexor Spasticity
- Affiliations
-
- 1Department of Rehabilitation Medicine and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Rehabilitation Medicine, Hansarang Asan General Hospital, Asan, Korea.
- 3Department of Rehabilitation Medicine, Inje University College of Medicine, Busan, Korea. bangik@sanggyepaik.ac.kr
- KMID: 1716526
- DOI: http://doi.org/10.3349/ymj.2005.46.4.546
Abstract
- Spasticity has been defined as a motor disorder characterized by a velocity-dependent increase in tonic stretch reflex (muscle tone). Muscle tone consists of mechanical-elastic characteristics, reflex muscle contraction and other elements. The aims of this study were to determine whether to assess spasticity quantitatively, and to characterize biomechanical and electromyographic spasticity assessment parameters. These assessment parameters were described by investigating the correlation between clinical measures and the response to passive sinusoidal movement with consecutive velocity increments. Twenty post-stroke hemiplegic patients and twenty normal healthy volunteers were included in the study. Five consecutive sinusoidal passive movements of the ankle were performed at specific velocities (60, 120, 180, and 240 degrees/ sec). We recorded the peak torque, work, and threshold angle using a computerized isokinetic dynamometer, and simultaneously measured the rectified integrated electromyographic activity. We compared these parameters both between groups and between different velocities. The peak torque, threshold angle, work, and rectified integrated electromyographic activity were significantly higher in the post-stroke spastic group at all angular velocities than in the normal control group. The threshold angle and integrated electromyographic activity increased significantly and linearly as angular velocity increased, but the peak torque and work were not increased in the post-stroke spastic group. Peak torque, work, and threshold angle were significantly correlated to the Modified Ashworth scale, but the integrated electromyographic activity was not. The biomechanical and electromyographic approach may be useful to quantitatively assess spasticity. However, it may also be very important to consider the different characteristics of each biomechanical parameter.
MeSH Terms
Figure
-

Fig. 1 Experiment setting for biomechanical assessment with electromyography of ankle plantar flexor spasticity.
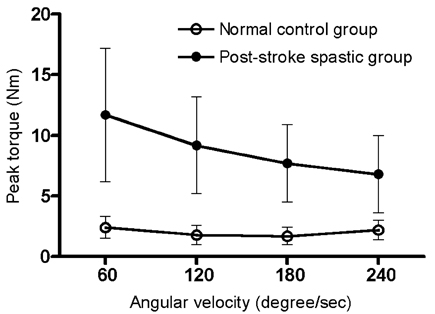
Fig. 2 Changes in peak torque with respect to angular velocity increments.

Fig. 3 Changes in work with respect to angular velocity increments.
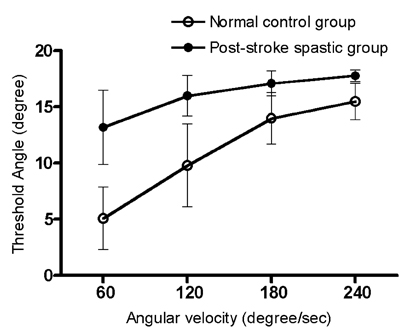
Fig. 4 Changes in threshold angle with respect to angular velocity increments.

Fig. 5 Changes in integrated electromyographic activity with respect to angular velocity Increments.
Reference
-
1. Lance JW. Feldman RG, Young RR, Koella WP, editors. Symposium Synopsis. Spasticity: Disordered motor control. 1980. 1st ed. Chicago: Year Book Publishers;485–494.2. Pinelli P, Villani A, Pasetti C, Pisano F, DiLorenzo G. Delwaide PJ, Young RR, editors. Electromyographic and kinesiological evaluation of spastic hemiplegic hand. Clinical neurophysiology in spasticity: contribution to assessment and pathophysiology. 1985. 1st ed. Amsterdam: Elserver;141–154.3. Wyke B. Neurological mechanisms in spasticity: a brief review of some current concepts. Physiotherapy. 1976. 62:316–319.4. Allison SC, Abraham LD. Correlation of quantitative measures with the modified Ashworth scale in the assessment of plantar flexor spasticity in patients with traumatic brain injury. J Neurol. 1995. 242:699–706.5. Benecke R, Conrad B, Meinck HM, Hohne J. Electromyographic analysis of bicycling on an ergometer for evaluation of spasticity of lower limbs in man. Adv Neurol. 1983. 39:1035–1046.6. Firoozbakhsh KK, Kunkel CF, Scremin AM, Moneim MS. Isokinetic dynamometric technique for spasticity assessment. Am J Phys Med Rehabil. 1993. 72:379–385.7. Lin JP, Brown JK, Brotherstone R. Assessment of spasticity in hemiplegic cerebral palsy. II: Distal lower-limb reflex excitability and function. Dev Med Child Neurol. 1994. 36:290–303.8. Skold C, Harms-Ringdahl K, Hultling C, Levi R, Seiger A. Simultaneous Ashworth measurements and electromyographic recordings in tetraplegic patients. Arch Phys Med Rehabil. 1998. 79:959–965.9. Bajd T, Vodovnik L. Pendulum testing of spasticity. J Biomed Eng. 1984. 6:9–16.10. Brown RA, Lawson DA, Leslie GC, Part NJ. Observations on the applicability of the Wartenberg pendulum test to healthy, elderly subjects. J Neurol Neurosurg Psychiatry. 1988. 51:1171–1177.11. Stillman B, McMeeken J. A video-based version of the pendulum test: technique and normal response. Arch Phys Med Rehabil. 1995. 76:166–176.12. Sloan RL, Sinclair E, Thompson J, Taylor S, Pentland B. Inter-rater reliability of the modified Ashworth Scale for spasticity in hemiplegic patients. Int J Rehabil Res. 1992. 15:158–161.13. Pandyan AD, Price CI, Barnes MP, Johnson GR. A biomechanical investigation into the validity of the modified Ashworth Scale as a measure of elbow spasticity. Clin Rehabil. 2003. 17:290–293.14. Katz RT, Rymer WZ. Spastic hypertonia: mechanisms and measurement. Arch Phys Med Rehabil. 1989. 70:144–155.15. Boiteau M, Malouin F, Richards CL. Use of a hand-held dynamometer and a Kin-Com dynamometer for evaluating spastic hypertonia in children: a reliability study. Phys Ther. 1995. 75:796–802.16. Gottlieb GL, Agarwal GC, Penn R. Sinusoidal oscillation of the ankle as a means of evaluating the spastic patient. J Neurol Neurosurg Psychiatry. 1978. 41:32–39.17. Lehmann JF, Price R, deLateur BJ, Hinderer S, Traynor C. Spasticity: quantitative measurements as a basis for assessing effectiveness of therapeutic intervention. Arch Phys Med Rehabil. 1989. 70:6–15.18. Allison SC, Abraham LD, Petersen CL. Reliability of the Modified Ashworth Scale in the assessment of plantarflexor muscle spasticity in patients with traumatic brain injury. Int J Rehabil Res. 1996. 19:67–78.19. O'Dwyer NJ, Ada L, Neilson PD. Spasticity and muscle contracture following stroke. Brain. 1996. 119:1737–1749.20. Skold C, Harms-Ringdahl K, Seiger A. Movement-provoked muscle torque and EMG activity in long-standing motor complete spinal cord injured individuals. J Rehabil Med. 2002. 34:86–90.21. Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987. 67:206–207.22. Corcos DM, Gottlieb GL, Penn RD, Myklebust B, Agarwal GC. Movement deficits caused by hyperexcitable stretch reflexes in spastic humans. Brain. 1986. 109:1043–1058.23. Akman MN, Bengi R, Karatas M, Kilinc S, Sozay S, Ozker R. Assessment of spasticity using isokinetic dynamometry in patients with spinal cord injury. Spinal Cord. 1999. 37:638–643.24. Engsberg JR, Olree KS, Ross SA, Park TS. Quantitative clinical measure of spasticity in children with cerebral palsy. Arch Phys Med Rehabil. 1996. 77:594–599.25. Given JD, Dewald JP, Rymer WZ. Joint dependent passive stiffness in paretic and contralateral limbs of spastic patients with hemiparetic stroke. J Neurol Neurosurg Psychiatry. 1995. 59:271–279.26. Katz RT, Rovai GP, Brait C, Rymer WZ. Objective quantification of spastic hypertonia: correlation with clinical findings. Arch Phys Med Rehabil. 1992. 73:339–347.27. Johnson GR. Outcome measures of spasticity. Eur J Neurol. 2002. 9:Suppl 1. 10–16. dicussion 53-61.28. Nuyens GE, De Weerdt WJ, Spaepen AJ Jr, Kiekens C, Feys HM. Reduction of spastic hypertonia during repeated passive knee movements in stroke patients. Arch Phys Med Rehabil. 2002. 83:930–935.29. Skold C. Spasticity in spinal cord injury: self- and clinically rated intrinsic fluctuations and intervention-induced changes. Arch Phys Med Rehabil. 2000. 81:144–149.30. Singer BJ, Dunne JW, Singer KP, Allison GT. Velocity dependent passive plantarflexor resistive torque in patients with acquired brain injury. Clin Biomech (Bristol, Avon). 2003. 18:157–165.31. Booth CM, Cortina-Borja MJ, Theologis TN. Collagen accumulation in muscles of children with cerebral palsy and correlation with severity of spasticity. Dev Med Child Neurol. 2001. 43:314–320.32. Katz RT. Rymer WZ, Katz RT, editors. Physical Medicine and Rehabilitaton: state of the art reviews on spasticity. Mechanisms of spastic hypertonia. 1994. 8th eds. Philadelphia: Hanley & Belfus, Inc;441–454.33. Damiano DL, Quinlivan JM, Owen BF, Payne P, Nelson KC, Abel MF. What does the Ashworth scale really measure and are instrumented measures more valid and precise? Dev Med Child Neurol. 2002. 44:112–118.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Passive Stretching on the Spasticity of Ankle Plantar Flexor Muscles
- A Quantitative Assessment of Spasticity in Hemiplegic Patients Using Isokinetic Dynamometer
- The Significance of Stretch Reflex Threshold Speed in Quantitative Assessment of Spasticity
- The Assessment of Spasticity Using Isokinetic Eccentric Torque Measurement
- Effects of Ankle Invertor and Plantar Flexor Stretching on Balance and Walking Ability of Stroke Patients
