Radiofrequency Ablation Combined with Transcatheter Arterial Chemoembolization for the Treatment of Single Hepatocellular Carcinoma of 2 to 5 cm in Diameter: Comparison with Surgical Resection
- Affiliations
-
- 1Department of Radiology, Chonnam National University Hwasun Hospital, Hwasun 519-763, Korea.
- 2Department of Radiology, Chonnam National University Medical School, Gwangju 501-757, Korea. kjradsss@dreamwiz.com
- 3Center for Aging and Geriatrics, Chonnam National University Medical School, Gwangju 501-757, Korea.
- 4Department of Internal Medicine, Chonnam National University Medical School, Gwangju 501-757, Korea.
- 5Department of Surgery, Chonnam National University Hwasun Hospital, Hwasun 519-763, Korea.
- KMID: 1715767
- DOI: http://doi.org/10.3348/kjr.2013.14.4.626
Abstract
OBJECTIVE
To compare the effectiveness of radiofrequency ablation (RFA) combined with transcatheter arterial chemoembolization (TACE) with surgical resection in patients with a single hepatocellular carcinoma (HCC) ranging from 2 to 5 cm.
MATERIALS AND METHODS
The study participants were enrolled over a period of 29 months and were comprised of 37 patients in a combined therapy group and 47 patients in a surgical resection group. RFA was performed the day after TACE, and surgical resection was performed by open laparotomy. The two groups were compared with respect to the length of hospital stay, rates of major complication, and rates of recurrence-free and overall survival.
RESULTS
Major complications occurred more frequently in the surgical resection group (14.9%) than in the combined therapy group (2.7%). However, there was no statistical significance (p = 0.059). The rates of recurrence-free survival at 1, 2, 3 and 4 years were similar between the combined therapy group (89.2%, 75.2%, 69.4% and 69.4%, respectively) and the surgical resection group (81.8%, 68.5%, 68.5% and 65%, respectively) (p = 0.7962, log-rank test). The overall survival rates at 1, 2, 3 and 4 years were also similar between groups (97.3%, 86.5%, 78.4% and 78.4%, respectively, in the combined therapy group, and 95.7%, 89.4%, 84.3% and 80.3%, respectively, in the surgical resection group) (p = 0.6321, log-rank test).
CONCLUSION
When compared with surgical resection for the treatment of a single HCC ranging from 2 to 5 cm, RFA combined with TACE shows similar results in terms of recurrence-free and overall survival rates.
Keyword
MeSH Terms
-
Carcinoma, Hepatocellular/diagnosis/mortality/*therapy
Catheter Ablation/*methods
Chemoembolization, Therapeutic/*methods
Disease-Free Survival
Female
Follow-Up Studies
Humans
Liver Neoplasms/diagnosis/mortality/*therapy
Male
Middle Aged
Neoplasm Recurrence, Local/epidemiology
Neoplasm Staging
Republic of Korea/epidemiology
Retrospective Studies
Survival Rate/trends
Treatment Outcome
Figure
-
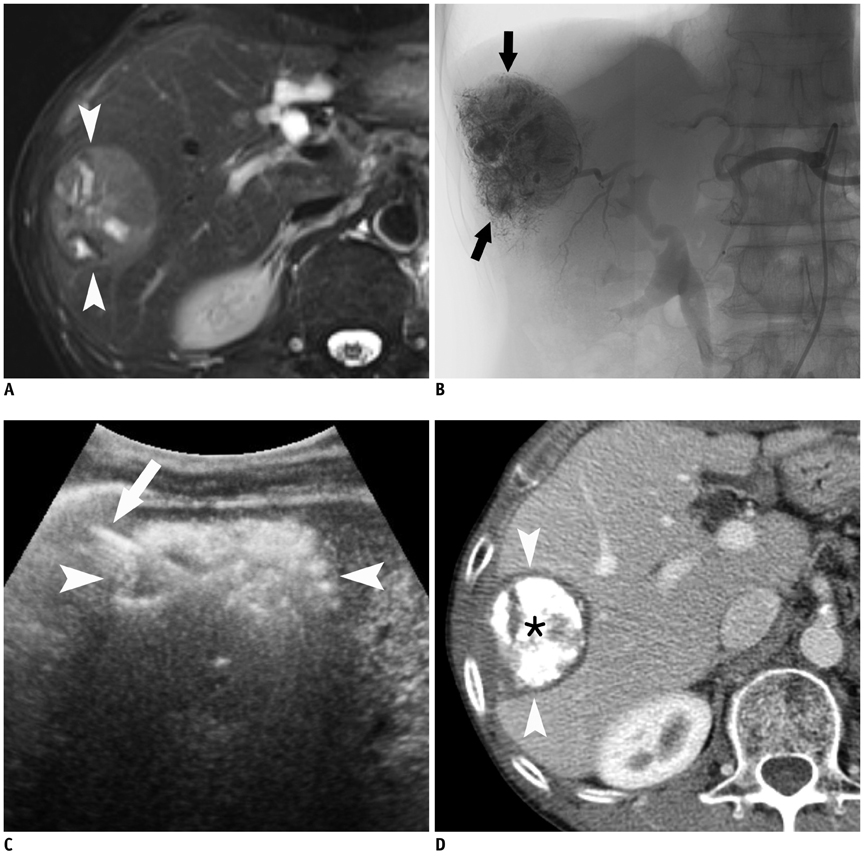
Fig. 1 Images of 59-year-old man with 5 cm non-infiltrating HCC, who underwent combined TACE and RFA. A. Fat-suppressed T2-weighted axial MR image obtained 1 week before combined treatment of TACE and RFA shows 5 cm heterogeneous hyperintense mass (arrowheads) in right hepatic lobe. B. Post-TACE angiogram shows dense radiopaque mass (arrows) with accumulated iodized oil in right hepatic lobe. C. US image during RFA shows mass surrounded by transient hyperechoic zone (arrowheads) and echogenic RF electrode (arrow) within mass. D. Contrast-enhanced CT image obtained 24 months after combined therapy shows dense iodized oil accumulation in mass (asterisk) surrounded by RF-induced coagulation (arrowheads), without local tumor progression. HCC = hepatocellular carcinoma, TACE = transcatheter arterial chemoembolization, RFA = radiofrequency ablation, US = ultrasonography
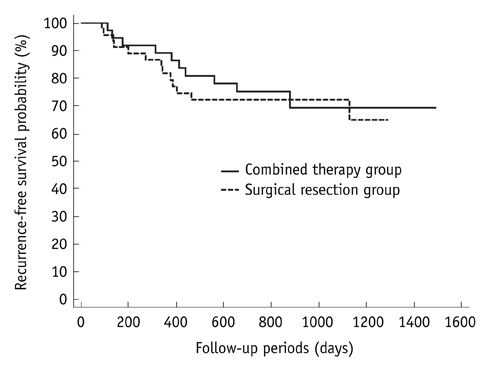
Fig. 2 Graph illustrates recurrence-free survival rates in patients with single hepatocellular carcinoma ranging from 2 to 5 cm treated with combined therapy or surgical resection. There was no significant difference between two groups (p = 0.7962, log-rank test).
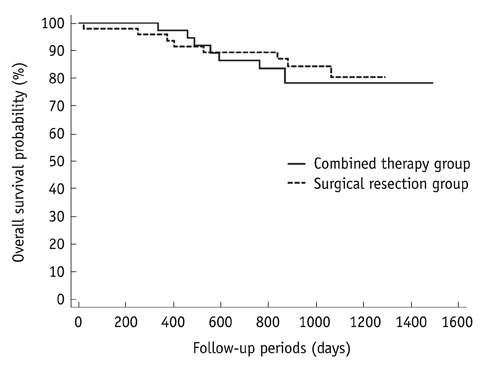
Fig. 3 Graph shows overall survival rates in patients with single hepatocellular carcinoma ranging from 2 to 5 cm treated with combined therapy or surgical resection. No significant difference was seen between two groups (p = 0.6321, log-rank test).
Cited by 2 articles
-
Efficacy and Safety of Combined Radiofrequency Ablation with Transarterial Chemoembolization in Patients with Barcelona Clinic Liver Cancer Stage A Hepatocellular Carcinoma Ineligible for Curative Treatment
Ah Ran Kim, Eugene Park, So Young Kwon, Seong Jun Park, Young Jung Kim, Byung Chul Yoo, Won Hyeok Choe, Jeong Han Kim, Jin Ho Hwang, Sang Woo Park, Young Jun Kim, Hee Sun Park, Mi hye Yu, Hae jeong Jeon
Korean J Gastroenterol. 2019;73(3):167-176. doi: 10.4166/kjg.2019.73.3.167.Radiofrequency Ablation Combined with Transcatheter Arterial Chemoembolization Therapy Versus Surgical Resection for Hepatocellular Carcinoma within the Milan Criteria: A Meta-Analysis
Wei-dong Wang, Li-hua Zhang, Jia-Yan Ni, Xiong-ying Jiang, Dong Chen, Yao-ting Chen, Hong-liang Sun, Jiang-hong Luo, Lin-feng Xu
Korean J Radiol. 2018;19(4):613-622. doi: 10.3348/kjr.2018.19.4.613.
Reference
-
1. Curley SA. Radiofrequency ablation of malignant liver tumors. Ann Surg Oncol. 2003; 10:338–347.2. Shibata T, Isoda H, Hirokawa Y, Arizono S, Shimada K, Togashi K. Small hepatocellular carcinoma: is radiofrequency ablation combined with transcatheter arterial chemoembolization more effective than radiofrequency ablation alone for treatment? Radiology. 2009; 252:905–913.3. Shibata T, Shibata T, Maetani Y, Isoda H, Hiraoka M. Radiofrequency ablation for small hepatocellular carcinoma: prospective comparison of internally cooled electrode and expandable electrode. Radiology. 2006; 238:346–353.4. Sutherland LM, Williams JA, Padbury RT, Gotley DC, Stokes B, Maddern GJ. Radiofrequency ablation of liver tumors: a systematic review. Arch Surg. 2006; 141:181–190.5. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Ierace T, Solbiati L, et al. Hepatocellular carcinoma: radio-frequency ablation of medium and large lesions. Radiology. 2000; 214:761–768.6. Seror O, N'Kontchou G, Ibraheem M, Ajavon Y, Barrucand C, Ganne N, et al. Large (>or=5.0-cm) HCCs: multipolar RF ablation with three internally cooled bipolar electrodes--initial experience in 26 patients. Radiology. 2008; 248:288–296.7. Yin XY, Xie XY, Lu MD, Xu HX, Xu ZF, Kuang M, et al. Percutaneous thermal ablation of medium and large hepatocellular carcinoma: long-term outcome and prognostic factors. Cancer. 2009; 115:1914–1923.8. Takaki H, Yamakado K, Nakatsuka A, Fuke H, Murata K, Shiraki K, et al. Radiofrequency ablation combined with chemoembolization for the treatment of hepatocellular carcinomas 5 cm or smaller: risk factors for local tumor progression. J Vasc Interv Radiol. 2007; 18:856–861.9. Livraghi T, Goldberg SN, Lazzaroni S, Meloni F, Solbiati L, Gazelle GS. Small hepatocellular carcinoma: treatment with radio-frequency ablation versus ethanol injection. Radiology. 1999; 210:655–661.10. Morimoto M, Sugimori K, Shirato K, Kokawa A, Tomita N, Saito T, et al. Treatment of hepatocellular carcinoma with radiofrequency ablation: radiologic-histologic correlation during follow-up periods. Hepatology. 2002; 35:1467–1475.11. Kagawa T, Koizumi J, Kojima S, Nagata N, Numata M, Watanabe N, et al. Transcatheter arterial chemoembolization plus radiofrequency ablation therapy for early stage hepatocellular carcinoma: comparison with surgical resection. Cancer. 2010; 116:3638–3644.12. Kang SG, Yoon CJ, Jeong SH, Kim JW, Lee SH, Lee KH, et al. Single-session combined therapy with chemoembolization and radiofrequency ablation in hepatocellular carcinoma less than or equal to 5 cm: a preliminary study. J Vasc Interv Radiol. 2009; 20:1570–1577.13. Kim JH, Won HJ, Shin YM, Kim SH, Yoon HK, Sung KB, et al. Medium-sized (3.1-5.0 cm) hepatocellular carcinoma: transarterial chemoembolization plus radiofrequency ablation versus radiofrequency ablation alone. Ann Surg Oncol. 2011; 18:1624–1629.14. Maluccio M, Covey AM, Gandhi R, Gonen M, Getrajdman GI, Brody LA, et al. Comparison of survival rates after bland arterial embolization and ablation versus surgical resection for treating solitary hepatocellular carcinoma up to 7 cm. J Vasc Interv Radiol. 2005; 16:955–961.15. Morimoto M, Numata K, Kondou M, Nozaki A, Morita S, Tanaka K. Midterm outcomes in patients with intermediate-sized hepatocellular carcinoma: a randomized controlled trial for determining the efficacy of radiofrequency ablation combined with transcatheter arterial chemoembolization. Cancer. 2010; 116:5452–5460.16. Rossi S, Garbagnati F, Lencioni R, Allgaier HP, Marchianò A, Fornari F, et al. Percutaneous radio-frequency thermal ablation of nonresectable hepatocellular carcinoma after occlusion of tumor blood supply. Radiology. 2000; 217:119–126.17. Yamakado K, Nakatsuka A, Takaki H, Yokoi H, Usui M, Sakurai H, et al. Early-stage hepatocellular carcinoma: radiofrequency ablation combined with chemoembolization versus hepatectomy. Radiology. 2008; 247:260–266.18. Kim JW, Kim JH, Won HJ, Shin YM, Yoon HK, Sung KB, et al. Hepatocellular carcinomas 2-3 cm in diameter: transarterial chemoembolization plus radiofrequency ablation vs. radiofrequency ablation alone. Eur J Radiol. 2012; 81:e189–e193.19. Helmberger T, Dogan S, Straub G, Schrader A, Jüngst C, Reiser M, et al. Liver resection or combined chemoembolization and radiofrequency ablation improve survival in patients with hepatocellular carcinoma. Digestion. 2007; 75:104–112.20. Bruix J, Sherman M. American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology. 2011; 53:1020–1022.21. Makuuchi M, Kosuge T, Takayama T, Yamazaki S, Kakazu T, Miyagawa S, et al. Surgery for small liver cancers. Semin Surg Oncol. 1993; 9:298–304.22. Goldberg SN, Grassi CJ, Cardella JF, Charboneau JW, Dodd GD 3rd, Dupuy DE, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria. J Vasc Interv Radiol. 2009; 20:7 Suppl. S377–S390.23. Okada S, Shimada K, Yamamoto J, Takayama T, Kosuge T, Yamasaki S, et al. Predictive factors for postoperative recurrence of hepatocellular carcinoma. Gastroenterology. 1994; 106:1618–1624.24. Takahashi S, Kudo M, Chung H, Inoue T, Ishikawa E, Kitai S, et al. Initial treatment response is essential to improve survival in patients with hepatocellular carcinoma who underwent curative radiofrequency ablation therapy. Oncology. 2007; 72:Suppl 1. 98–103.25. Buscarini E, Savoia A, Brambilla G, Menozzi F, Reduzzi L, Strobel D, et al. Radiofrequency thermal ablation of liver tumors. Eur Radiol. 2005; 15:884–894.26. Goldberg SN, Girnan GD, Lukyanov AN, Ahmed M, Monsky WL, Gazelle GS, et al. Percutaneous tumor ablation: increased necrosis with combined radio-frequency ablation and intravenous liposomal doxorubicin in a rat breast tumor model. Radiology. 2002; 222:797–804.27. Veltri A, Moretto P, Doriguzzi A, Pagano E, Carrara G, Gandini G. Radiofrequency thermal ablation (RFA) after transarterial chemoembolization (TACE) as a combined therapy for unresectable non-early hepatocellular carcinoma (HCC). Eur Radiol. 2006; 16:661–669.28. Komorizono Y, Oketani M, Sako K, Yamasaki N, Shibatou T, Maeda M, et al. Risk factors for local recurrence of small hepatocellular carcinoma tumors after a single session, single application of percutaneous radiofrequency ablation. Cancer. 2003; 97:1253–1262.29. Mazzaferro V, Battiston C, Perrone S, Pulvirenti A, Regalia E, Romito R, et al. Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann Surg. 2004; 240:900–909.30. Kim YS, Lee WJ, Rhim H, Lim HK, Choi D, Lee JY. The minimal ablative margin of radiofrequency ablation of hepatocellular carcinoma (> 2 and < 5 cm) needed to prevent local tumor progression: 3D quantitative assessment using CT image fusion. AJR Am J Roentgenol. 2010; 195:758–765.31. Lam VW, Ng KK, Chok KS, Cheung TT, Yuen J, Tung H, et al. Incomplete ablation after radiofrequency ablation of hepatocellular carcinoma: analysis of risk factors and prognostic factors. Ann Surg Oncol. 2008; 15:782–790.32. Park MJ, Kim YS, Rhim H, Lim HK, Lee MW, Choi D. A comparison of US-guided percutaneous radiofrequency ablation of medium-sized hepatocellular carcinoma with a cluster electrode or a single electrode with a multiple overlapping ablation technique. J Vasc Interv Radiol. 2011; 22:771–779.33. Lee J, Lee JM, Yoon JH, Lee JY, Kim SH, Lee JE, et al. Percutaneous radiofrequency ablation with multiple electrodes for medium-sized hepatocellular carcinomas. Korean J Radiol. 2012; 13:34–43.34. Kang TW, Rhim H, Kim EY, Kim YS, Choi D, Lee WJ, et al. Percutaneous radiofrequency ablation for the hepatocellular carcinoma abutting the diaphragm: assessment of safety and therapeutic efficacy. Korean J Radiol. 2009; 10:34–42.35. Rhim H, Lim HK, Kim YS, Choi D. Percutaneous radiofrequency ablation with artificial ascites for hepatocellular carcinoma in the hepatic dome: initial experience. AJR Am J Roentgenol. 2008; 190:91–98.36. Ahrar K, Newman RA, Pang J, Vijjeswarapu MK, Wallace MJ, Wright KC. 2004 Dr. Gary J. Becker Young Investigator Award: Relative thermosensitivity of cytotoxic drugs used in transcatheter arterial chemoembolization. J Vasc Interv Radiol. 2004; 15:901–905.37. Guang C, Kawai N, Sato M, Takasaka I, Minamiguchi H, Sahara S, et al. Effect of interval between transcatheter hepatic arterial embolization and radiofrequency ablation on ablated lesion size in a swine model. Jpn J Radiol. 2011; 29:649–655.38. Lupo L, Panzera P, Giannelli G, Memeo M, Gentile A, Memeo V. Single hepatocellular carcinoma ranging from 3 to 5 cm: radiofrequency ablation or resection? HPB (Oxford). 2007; 9:429–434.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Chemoembolization combined with radiofrequency ablation is the best option for the local treatment of early hepatocellular carcinoma?
- Effect of Ultrasound-Guided Radiofrequency Ablation in Incompletely Treated Hepatocellular Carcinoma after Transcatheter Arterial Chemoembolization
- Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
- The Role of Combination of Transarterial Chemoebolization and Radiofrequency Ablation for Hepatocellular Carcinoma Treatment
- Efficacy of Hepatic Arterial Infusion Chemotherapy and Radiofrequency Ablation against Hepatocellular Carcinoma Refractory to Transarterial Chemoembolization and Vascular Variation: A Case Study
