Imaging Spectrum after Pancreas Transplantation with Enteric Drainage
- Affiliations
-
- 1Department of Radiology, Taichung Veterans General Hospital, Taichung 40705, Taiwan.
- 2Department of Radiology, Taipei Veterans General Hospital, Taipei 11217, Taiwan. rclee@vghtpe.gov.tw
- 3National Yang-Ming University School of Medicine, Taipei 11221, Taiwan.
- 4Department of Surgery, Taipei Veterans General Hospital, Taipei 11217, Taiwan.
- KMID: 1711476
- DOI: http://doi.org/10.3348/kjr.2014.15.1.45
Abstract
- Since the introduction of pancreas transplantation more than 40 years ago, surgical techniques and immunosuppressive regiments have improved and both have contributed to increase the number and success rate of this procedure. However, graft survival corresponds to early diagnosis of organ-related complications. Thus, knowledge of the transplantation procedure and postoperative image anatomy are basic requirements for radiologists. In this article, we demonstrate the imaging spectrum of pancreas transplantation with enteric exocrine drainage.
Keyword
MeSH Terms
-
Adult
Anastomosis, Surgical/methods
Diagnostic Imaging/methods
Drainage/methods
Female
Graft Rejection/pathology
Graft Survival
Humans
Iliac Artery/radiography/surgery
Immunosuppressive Agents
Kidney Transplantation
Male
*Medical Illustration
Mesenteric Artery, Superior/radiography/surgery
Middle Aged
Pancreas/*blood supply/radiography
Pancreas Transplantation/adverse effects/*methods
Pancreatitis, Graft/etiology
Portal Vein/radiography/surgery
Postoperative Complications/radiography
Postoperative Hemorrhage/etiology
Survival Rate
Immunosuppressive Agents
Figure
-
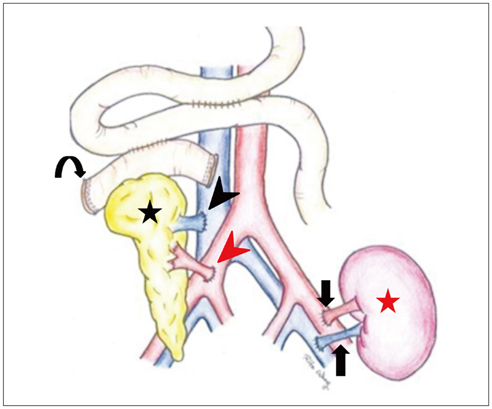
Fig. 1 Pancreas is typically placed in right lower intraperitoneal cavity or pelvis, and kidney is placed on left during simultaneous pancreas-kidney transplantation. Common iliac artery portion of Y-graft (red arrowhead) is anastomosed to recipient's common iliac artery or external iliac artery. Donor superior mesenteric vein (black arrowhead) is anastomosed to distal inferior vena cava in systemic drainage (curved arrow, donor duodenum; black star, pancreas; red star, kidney; arrows, renal vessels).
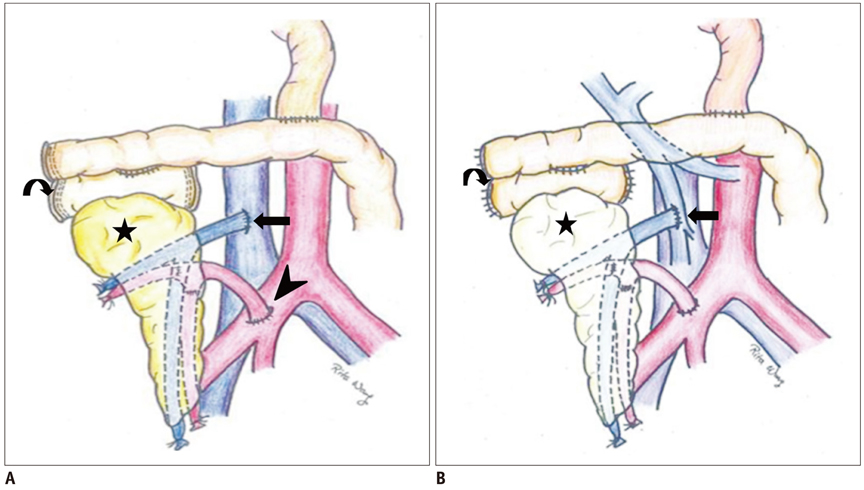
Fig. 2 Illustration of pancreas transplantation alone. A. With systemic venous revasculization (arrow, anastomosis of graft superior mesenteric vein [SMV] to inferior vena cava [IVC]; arrowhead, anastomosis of donor Y-graft to common or external iliac artery). B. With portal venous revascularization (arrow, anastomosis of graft SMV to major branch of recipient SMV). Both procedures are performed with enteric exocrine drainage (curved arrow, donor duodenum; black star, pancreas).
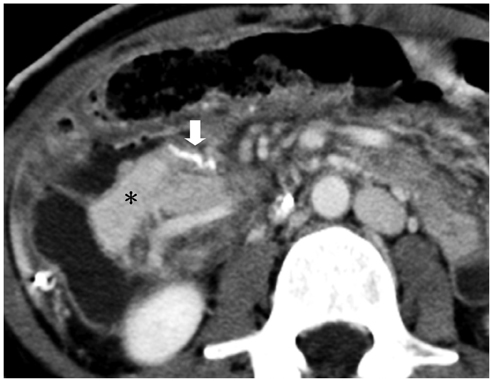
Fig. 3 Stapling device. Stapling devices are usually used for both proximal and distal ends of donor duodenum, and these radiodense devices may offer good landmarks to localize duodenum and pancreatic head quickly on computed tomography scan (white arrow, surgical staples; star, pancreas head).
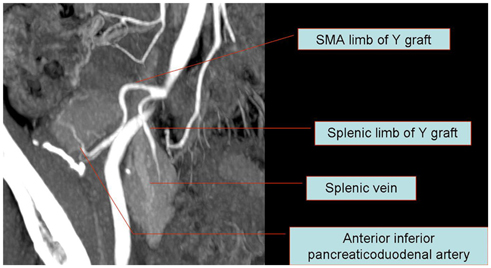
Fig. 4 Anatomy of Y-graft with two limbs anastomosed with superior mesenteric vein and splenic artery. After harvesting allograft from donor, arterial "Y-graft" is prepared on "back-table" with donor common iliac, internal, and external iliac arteries. Donor superior mesenteric artery (SMA) is anastomosed to donor external iliac artery limb of Y-graft, and donor splenic artery is anastomosed to donor internal iliac artery limb of Y-graft. Common iliac artery portion is then anastomosed to recipient's common iliac artery or external iliac artery.
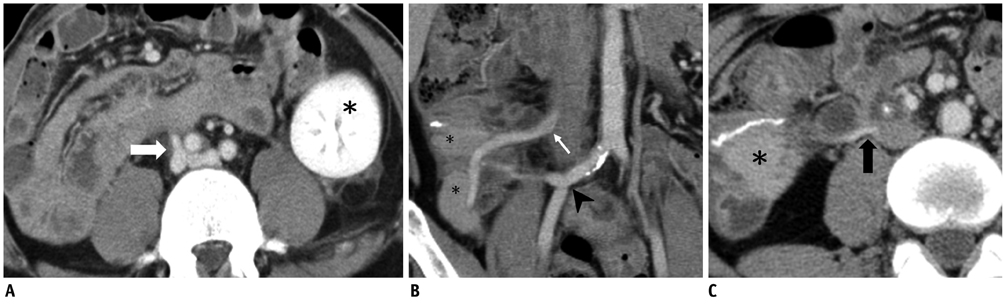
Fig. 5 Normal venous graft appearance. A. 33-year-old man with simultaneous pancreas-kidney transplantation. Normal venous graft appearance and anastomosis of donor superior mesenteric vein (SMV) to right iliac vein (arrow) is shown on axial computed tomography (CT) view (star, graft kidney). B, C. 41-year-old man with pancreatic transplantation alone. Patent venous graft sometimes appears collapsed on CT, yet it is patent (star, pancreas; white arrow in B and black arrow in C; anastomosis of donor SMV to inferior vena cava; arrowhead, anastomosis of Y-graft to recipient right iliac artery).
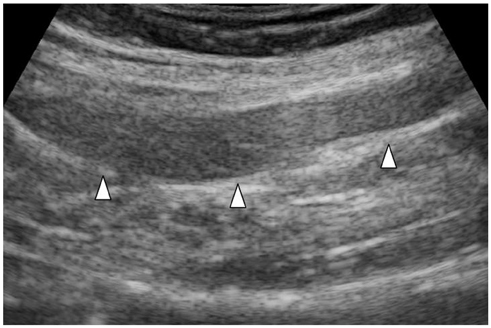
Fig. 6 Normal pancreatic grafts appear hypoechoic to surrounding omental or mesenteric fat and show homogeneous echotexture (white arrowheads).

Fig. 7 51-year-old male with pancreas necrosis 2 weeks after simultaneous pancreas-kidney transplantation. Computed tomography shows absence of parenchymal enhancement, diffuse enlargement of graft wrapping around graft kidney, and poor graft vascular opacification (white arrows, necrotic pancreas, curved arrow, surgical staple line). He finally received graft pancreatectomy. Note that graft kidney (black star) is normal.

Fig. 8 29-year-old female after simultaneous pancreas-kidney transplantation with thrombosis in donor splenic vein and superior mesenteric vein. A. Non-contrast axial computed tomography (CT) scan was performed 8 days after operation (arrows, thrombus). B. Contrast-enhanced CT was performed 3 weeks after operation. Persistent thrombosis within donor veins was seen (white arrows, thrombus; black triangles, pancreas; black star, kidney).
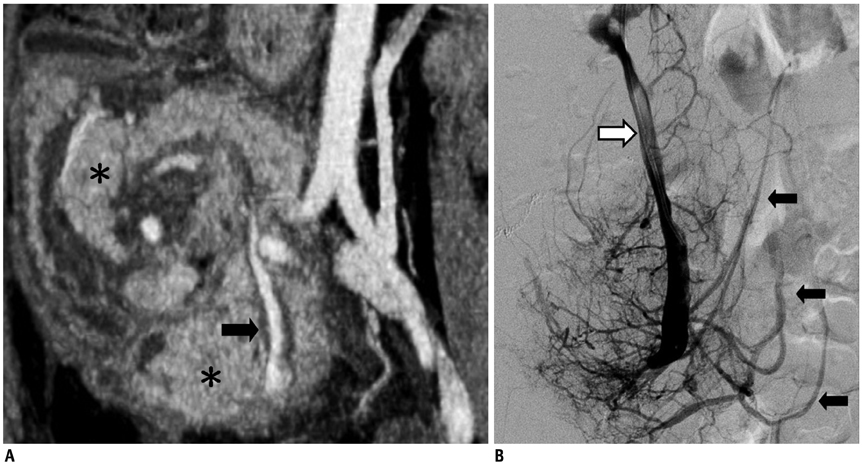
Fig. 9 31-year-old female 11 days after pancreatic transplantation. A. Computed tomography scan shows venous thrombosis (arrow, filling defect in donor splenic vein; white star, pancreas). B. Angiography confirmed presence of thrombus in donor splenic vein. However, endocrine function of graft pancreas was clinically normal. Increased collateral venous network had developed (black arrows), which probably preserved pancreatic graft from venous thrombotic pancreatitis (white arrow, thrombus in donor splenic vein).
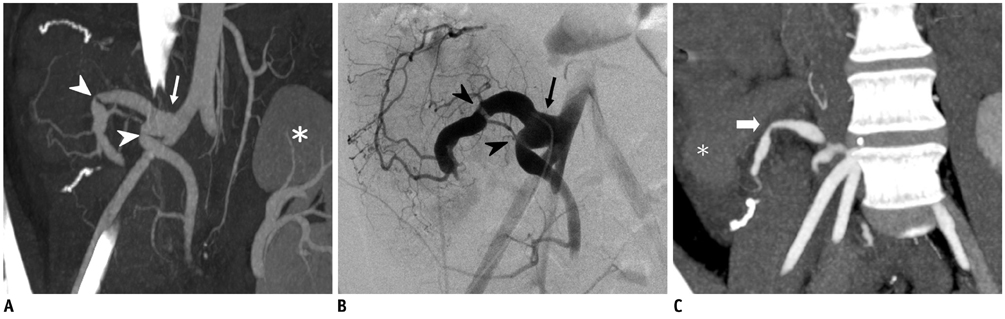
Fig. 10 31-year-old female 11 days after pancreatic transplantation. Maximal intensity projection image from computed tomography angiography (A) shows kinking of Y-graft, which was confirmed on angiography (B). However, blood supply to both limbs of Y-graft and endocrine function of graft were normal (arrow, patent Y-graft; arrowheads, kinking of both limbs; star, kidney). C. Superior mesenteric artery limb and splenic artery limb showed progressive narrowing 1 year later, yet perfusion and endocrine function of graft pancreas remained normal. Angioplasty is considered only when there is significant hemodynamic impairment concomitant with graft dysfunction (arrow, kinking sites with narrowing; star, pancreatic head).

Fig. 11 20-year-old male after pancreatic transplantation alone. One year after operation (A) computed tomography (CT) scan shows mild swelling of pancreas (star) and (B) ultrasound-guided biopsy proved mild rejection. Swelling of pancreas with hypoechoic echogenicity was noted (white star). C. Follow-up CT scan 3 years after operation showed significant atrophy of pancreas. However, endocrine function of graft pancreas was normal (arrowheads, atrophic pancreas; arrow, donor duodenum with surgical staples).
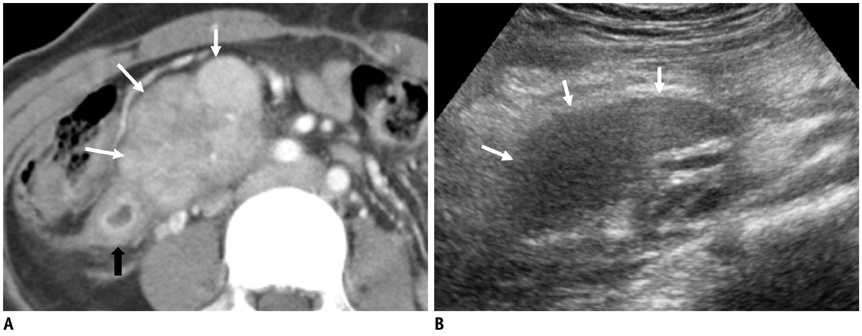
Fig. 12 37-year-old female with pancreatic transplantation alone. She presented with markedly elevated pancreatic enzymes 16 months after operation. A. Contrast-enhanced computed tomography (CT) showed swelling of pancreatic head with heterogeneous contrast enhancement (white arrows) and duodenal wall edema (black arrow) indicating pancreatitis. B. Gray-scale ultrasound also revealed swollen hypoechoic pancreatic head (white arrows) and biopsy proven acute rejection. We cannot distinguish rejection from pancreatitis on contrast-enhanced CT scan or ultrasound images, and biopsy is only way to confirm this diagnosis.
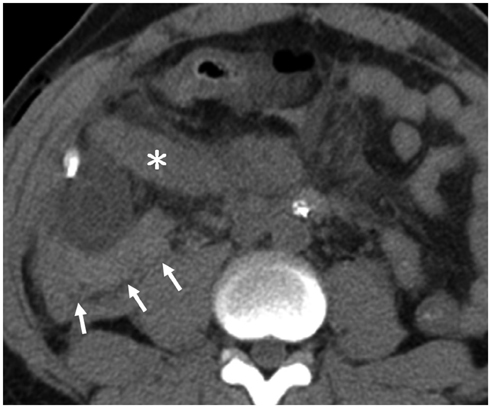
Fig. 13 43-year-old male 1 day after simultaneous pancreas-kidney transplantation. Hematoma was seen on non-contrast computed tomography scan (star, pancreas; arrows, hematoma). He underwent exploratory laparotomy to check for bleeder and to remove hematoma.
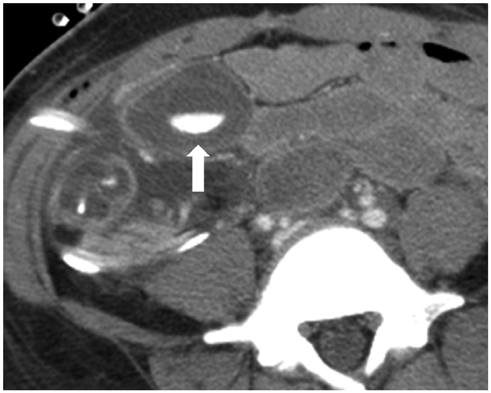
Fig. 14 34-year-old female 2 days after pancreatic transplantation alone. Computed tomography scan showed active bleeding (arrow) of Roux-limb of intestine. Bleeding subsided after conservative treatment.
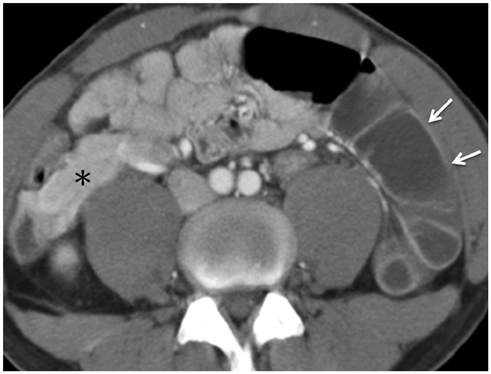
Fig. 15 30-year-old male after pancreatic transplantation alone. Intestinal obstruction with adhesion band is noted 8 months after operation (arrows, fluid-filled dilated bowel loops; star, pancreas).

Fig. 16 26-year-old female after pancreatic transplantation alone. Biopsy was performed intraoperatively because donor had systemic lupus erythematosus. Computed tomography scan 1 week after operation showed fluid collection around graft pancreas (arrow) and exploratory laparotomy revealed pancreatic juice leakage from biopsy site.
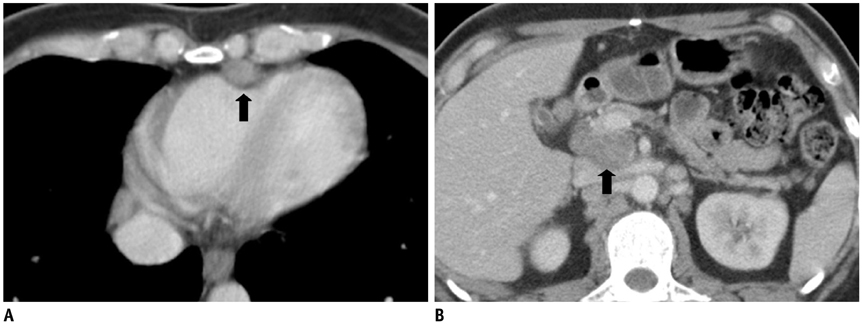
Fig. 17 33-year-old male after pancreatic transplantation alone. Multiple soft tissue nodules in mediastinum (A, black arrow) and abdomen (B, black arrow) are noted on contrast-enhanced computed tomography 15 months after transplantation. Biopsy of neck lymph nodes proved Kaposi's sarcoma and HHV-8 positivity.

Fig. 18 25-year-old female after simultaneous pancreas-kidney transplantation with hepatic veno-occlusive disease. Patient presented 9 months after operation with elevated liver enzymes and jaundice. Contrast-enhanced computed tomography (CT) scan showed pericardial effusion (A), hepatomegaly with heterogeneous race-like enhancement of hepatic parenchyma, periportal edema, and ascites (B). Surgeon shifted her immunosuppressant from tacrolimus to cyclosporine, and CT after 3 months revealed significant resolution of abnormal findings seen in previous study.
Reference
-
1. Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC. Allotransplantation of the pancreas and duodenum along with the kidney in diabetic nephropathy. Surgery. 1967; 61:827–837.2. Baktavatsalam R, Little DM, Connolly EM, Farrell JG, Hickey DP. Complications relating to the urinary tract associated with bladder-drained pancreatic transplantation. Br J Urol. 1998; 81:219–223.3. Vandermeer FQ, Manning MA, Frazier AA, Wong-You-Cheong JJ. Imaging of whole-organ pancreas transplants. Radiographics. 2012; 32:411–435.4. Hagspiel KD, Nandalur K, Pruett TL, Leung DA, Angle JF, Spinosa DJ, et al. Evaluation of vascular complications of pancreas transplantation with high-spatial-resolution contrast-enhanced MR angiography. Radiology. 2007; 242:590–599.5. Freund MC, Steurer W, Gassner EM, Unsinn KM, Rieger M, Koenigsrainer A, et al. Spectrum of imaging findings after pancreas transplantation with enteric exocrine drainage: Part 2, posttransplantation complications. AJR Am J Roentgenol. 2004; 182:919–925.6. Chandra J, Phillips RR, Boardman P, Gleeson FV, Anderson EM. Pancreas transplants. Clin Radiol. 2009; 64:714–723.7. Margreiter C, Mark W, Wiedemann D, Sucher R, Ollinger R, Bösmüller C, et al. Pancreatic graft survival despite partial vascular graft thrombosis due to splenocephalic anastomoses. Am J Transplant. 2010; 10:846–851.8. Drachenberg CB, Papadimitriou JC. Spectrum of histopathological changes in pancreas allograft biopsies and relationship to graft loss. Transplant Proc. 2007; 39:2326–2328.9. Holalkere NS, Soto J. Imaging of miscellaneous pancreatic pathology (trauma, transplant, infections, and deposition). Radiol Clin North Am. 2012; 50:515–528.10. Dillman JR, Elsayes KM, Bude RO, Platt JF, Francis IR. Imaging of pancreas transplants: postoperative findings with clinical correlation. J Comput Assist Tomogr. 2009; 33:609–617.11. Atwell TD, Gorman B, Larson TS, Charboneau JW, Ingalls Hanson BM, Stegall MD. Pancreas transplants: experience with 232 percutaneous US-guided biopsy procedures in 88 patients. Radiology. 2004; 231:845–849.12. Nelson NL, Largen PS, Stratta RJ, Taylor RJ, Grune MT, Hapke MR, et al. Pancreas allograft rejection: correlation of transduodenal core biopsy with Doppler resistive index. Radiology. 1996; 200:91–94.13. Aideyan OA, Foshager MC, Benedetti E, Troppmann C, Gruessner RW. Correlation of the arterial resistive index in pancreas transplants of patients with transplant rejection. AJR Am J Roentgenol. 1997; 168:1445–1447.14. Shyr YM, Su CH, Li AF, Wu CW, Lui WY. Canine pancreas allotransplantation with enteric drainage. Zhonghua Yi Xue Za Zhi (Taipei). 2002; 65:483–488.15. Farge D. Kaposi’s sarcoma in organ transplant recipients. The Collaborative Transplantation Research Group of Ile de France. Eur J Med. 1993; 2:339–334.16. Wadleigh M, Ho V, Momtaz P, Richardson P. Hepatic venoocclusive disease: pathogenesis, diagnosis and treatment. Curr Opin Hematol. 2003; 10:451–462.
