Malignant Extrarenal Rhabdoid Tumor in Adults: Three Case Reports Originating from the Ileum, Adrenal Gland and Uterus
- Affiliations
-
- 1Department of Radiology, Ansan Hospital, Korea University College of Medicine, Ansan, Korea. pagoda20@gmail.com
- 2Department of Colorectal Surgery, Ansan Hospital, Korea University College of Medicine, Ansan, Korea.
- 3Department of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Pathology, Ansan Hospital, Korea University College of Medicine, Ansan, Korea.
- KMID: 1709016
- DOI: http://doi.org/10.3348/jksr.2014.71.1.20
Abstract
- Malignant extrarenal rhabdoid tumor (MERT) is a very aggressive tumor that is extremely rare in adults. Herein, we introduce three cases of MERT in adults that originated in the ileum, adrenal gland, and uterine endometrium. The MERTs in the ileum and adrenal gland showed non-aggressive features and a good prognosis, while the MERT in the uterine presented with aggressive features and distant metastasis.
MeSH Terms
Figure
-

Fig. 1 A 52-year-old woman suffered from cramping abdominal pain. A. A 70-second-delayed contrast-enhanced coronal CT scan shows a well-enhanced mass (arrowheads) in the distal ileum. The mass has an intraluminal protruding appearance and no luminal obstruction. B. On 5 days from initial study, contrast enema with water-soluble contrast medium (Gastrografin) is performed due to recurred pain. It shows an ileocolic type intussusception (arrowheads). C. The intussusception (arrowheads) is moved proximally to the distal ileum with the pressure of the enema, but not completely resolved. D. The mass (M) is protruding at the mucosal surface, and the cut surface of the tumor is pale yellow, invading the muscular layer (arrow) and sparing the adventitia (arrowhead) macroscopically. E. In a low-power field-microscopic photograph (H&E stain, × 40), the tumor penetrates the entire proper muscle (PM) layer (arrowhead), and lymphatic tumor emboli are noted. F. In a high-power field-microscopic photograph (H&E stain, × 400), the tumor is composed of polygonal and loosely cohesive cells. The cells show large, eccentric nuclei, homogenous eosinophilic cytoplasm, and intra-cytoplasmic inclusions (arrows), concordant with rhabdoid cells.

Fig. 2 A 63-year-old man presenting a right adrenal gland mass. A. A pre-enhanced CT scan shows well-defined, round-shaped, low attenuatting mass in the right upper abdominal cavity. B. An 120-second-delayed contrast-enhanced CT scan shows poor enhancement of the mass. The mass is positioned at a blunt angle to the right adrenal gland (arrowheads). C. The cut surface of the tumor is pinkish tan and soft with hemorrhagic and myxoid foci.
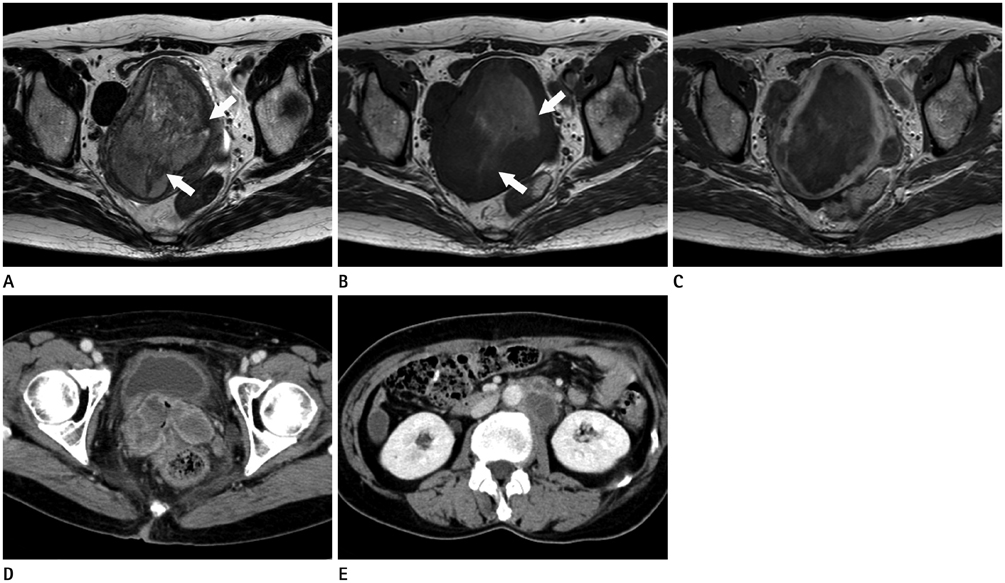
Fig. 3 A 58-year-old woman complaining vaginal spotting. A, B. The uterine endometrial mass presents with heterogeneous high-signal intensity on T2-weighted image (A) and heterogeneous low-signal intensity on T1-weighted image (B). Multiple T2 low-signal and T1 high-signal intensity foci in the mass, representing hemorrhage (arrows). C. Contrast-enhanced T1-weighted MR image shows poor enhancement of the mass. D, E. Contrast-enhanced CT scan images performed 3 months after the operation show multiple pelvic tumors and retroperitoneal lymphadenopathy.
Reference
-
1. Abdullah A, Patel Y, Lewis TJ, Elsamaloty H, Strobel S. Extrarenal malignant rhabdoid tumors: radiologic findings with histopathologic correlation. Cancer Imaging. 2010; 10:97–101.2. Haas JE, Palmer NF, Weinberg AG, Beckwith JB. Ultrastructure of malignant rhabdoid tumor of the kidney. A distinctive renal tumor of children. Hum Pathol. 1981; 12:646–657.3. Biegel JA, Kalpana G, Knudsen ES, Packer RJ, Roberts CW, Thiele CJ, et al. The role of INI1 and the SWI/SNF complex in the development of rhabdoid tumors: meeting summary from the workshop on childhood atypical teratoid/rhabdoid tumors. Cancer Res. 2002; 62:323–328.4. Gadd S, Sredni ST, Huang CC, Perlman EJ. Renal Tumor Committee of the Children's Oncology Group. Rhabdoid tumor: gene expression clues to pathogenesis and potential therapeutic targets. Lab Invest. 2010; 90:724–738.5. Ogino S, Ro TY, Redline RW. Malignant rhabdoid tumor: A phenotype? An entity?--A controversy revisited. Adv Anat Pathol. 2000; 7:181–190.6. Fanburg-Smith JC, Hengge M, Hengge UR, Smith JS Jr, Miettinen M. Extrarenal rhabdoid tumors of soft tissue: a clinicopathologic and immunohistochemical study of 18 cases. Ann Diagn Pathol. 1998; 2:351–362.7. Tóth L, Nemes Z, Gomba S, Asztalos L, Molnár C, András C, et al. Primary rhabdoid cancer of the ileum: a case report and review of the literature. Pathol Res Pract. 2010; 206:110–115.8. Salamanca J, Nevado M, Martínez-González MA, Pérez-Espejo G, Pinedo F. Undifferentiated carcinoma of the jejunum with extensive rhabdoid features. Case report and review of the literature. APMIS. 2008; 116:941–946.9. Yaris N, Cobanoglu U, Dilber E, Ahmetoğlu A, Saruhan H, Okten A. Malignant rhabdoid tumor of adrenal gland. Med Pediatr Oncol. 2002; 39:128–131.10. Horazdovsky R, Manivel JC, Cheng EY. Successful salvage and long-term survival after recurrent malignant rhabdoid tumor. Sarcoma. 2007; 2007:53549.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Extrarenal Rhabdoid Tumor of the Retroperitoneum
- Imaging Findings of a Malignant Rhabdoid Tumor in the Stomach: A Case Report
- A Case of Malignant Extrarenal Rhabdoid Tumor
- A Case of Malignant Rhabdoid Tumor on the Face
- Malignant Extrarenal Rhabdoid Tumor of the Pelvic Paravertebral Region: Case Report
