Cataracts among Adults Aged 30 to 49 Years: A 10-Year Study from 1995 to 2004 in Korea
- Affiliations
-
- 1Department of Ophthalmology and Visual Science, St. Mary's Hospital, The Catholic University of Korea, College of Medicine, Seoul, Korea. eyedoc@catholic.ac.kr
- KMID: 1707288
- DOI: http://doi.org/10.3341/kjo.2013.27.5.345
Abstract
- PURPOSE
To investigate the long-term characteristics of cataracts among adults aged 30 to 49 years in Korean over a span of 10 years.
METHODS
Subjects between the ages of 30 to 49 years who underwent cataract surgery at St. Mary's Hospital from 1995 to 2004 (n = 976) were included. Patients with a history of ocular trauma, uveitis, other ocular or systemic diseases, and congenital cataracts were excluded. Additional information including type of lens opacity, urban/rural region, and pre- and postoperative visual acuities were analyzed. Lens opacity grading was conducted using Lens Opacity Classification System III. The Cochran-Armitage proportion trend test was used to analyze vision changes with the passage of time.
RESULTS
Among the patients who had undergone cataract surgeries, 8.8% (976 / 11,111) met the inclusion criteria. The mean age was 41.7 +/- 5.45 years. Gender breakdown of the patient population included 79.0% male and 21.0% female. In terms of home environment, 60.9% were from an urban region and 39.1% from a rural region. Opacity type included anterior polar (AP), posterior subcapsular (PSC), AP and PSC, cortical, and nuclear in 35.7%, 35.1%, 7.0%, 6.0%, and 5.4% of patients, respectively. At a 2-month postoperative follow-up appointment, 92.7% of patients showed a best-corrected visual acuity of more than 20 / 40.
CONCLUSIONS
Predominance of AP and PSC opacities as well as male patients was observed in this study population.
MeSH Terms
Figure
-
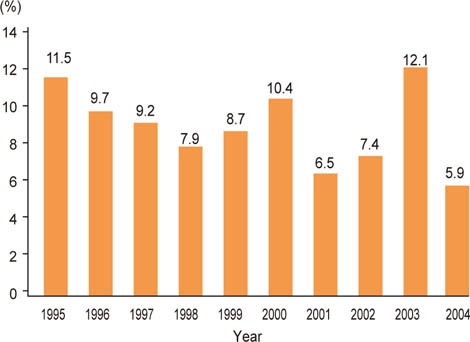
Fig. 1 Changes of the proportion of adults with cataracts aged 30 to 49 years over 10 years. The proportion of adults aged from 30 to 49 years who underwent cataract surgery displayed statistically significant decrease in the prevalence of cataracts as time progressed (Cochran-Armitage test, p = 0.0002).

Fig. 2 The proportion of each type of lens opacity in adults aged from 30 to 49 years who underwent cataract surgery. Anterior polar (AP) opacity (35.7%, 348 / 976) and posterior subcapsular (PSC) opacity (35.1%, 343 / 976) were the most common type of lens opacity among all subjects. Mixed AP and PSC opacities (7.0%, 68 / 976) were more common than cortical opacities (6.0%, 59 / 976) alone or nuclear opacities (5.4%, 53 / 976) alone. Mixed nuclear and cortical type lens opacities accounted for 10.8% (105 / 976) of the total opacity types. CO = cortical opacity; NO = nuclear opacity.
Reference
-
1. Hu TS, Zhen Q, Sperduto RD, et al. Age-related cataract in the Tibet Eye Study. Arch Ophthalmol. 1989; 107:666–669.2. Seah SK, Wong TY, Foster PJ, et al. Prevalence of lens opacity in Chinese residents of Singapore: the tanjong pagar survey. Ophthalmology. 2002; 109:2058–2064.3. West SK, Munoz B, Schein OD, et al. Racial differences in lens opacities: the Salisbury Eye Evaluation (SEE) project. Am J Epidemiol. 1998; 148:1033–1039.4. Leske MC, Connell AM, Wu SY, et al. Prevalence of lens opacities in the Barbados Eye Study. Arch Ophthalmol. 1997; 115:105–111.5. Sperduto RD, Hiller R. The prevalence of nuclear, cortical, and posterior subcapsular lens opacities in a general population sample. Ophthalmology. 1984; 91:815–818.6. Adamsons I, Munoz B, Enger C, Taylor HR. Prevalence of lens opacities in surgical and general populations. Arch Ophthalmol. 1991; 109:993–997.7. Klein BE, Klein R, Linton KL. Prevalence of age-related lens opacities in a population. The Beaver Dam Eye Study. Ophthalmology. 1992; 99:546–552.8. Mitchell P, Cumming RG, Attebo K, Panchapakesan J. Prevalence of cataract in Australia: the Blue Mountains eye study. Ophthalmology. 1997; 104:581–588.9. Xu L, Cui T, Zhang S, et al. Prevalence and risk factors of lens opacities in urban and rural Chinese in Beijing. Ophthalmology. 2006; 113:747–755.10. Tsai SY, Hsu WM, Cheng CY, et al. Epidemiologic study of age-related cataracts among an elderly Chinese population in Shih-Pai, Taiwan. Ophthalmology. 2003; 110:1089–1095.11. Husain R, Tong L, Fong A, et al. Prevalence of cataract in rural Indonesia. Ophthalmology. 2005; 112:1255–1262.12. Song KJ, Han MY, Kim SY, et al. Prevalence estimation of cataract based on a screening test. J Korean Ophthalmol Soc. 2007; 48:768–773.13. Yoon KC, Mun GH, Kim SD, et al. Prevalence of eye diseases in South Korea: data from the Korea National Health and Nutrition Examination Survey 2008-2009. Korean J Ophthalmol. 2011; 25:421–433.14. Zetterström C, Lundvall A, Kugelberg M. Cataracts in children. J Cataract Refract Surg. 2005; 31:824–840.15. Jain IS, Pillay P, Gangwar DN, et al. Congenital cataract: etiology and morphology. J Pediatr Ophthalmol Strabismus. 1983; 20:238–242.16. Bardelli AM, Lasorella G, Vanni M. Congenital and developmental cataracts and multimalformation syndromes. Ophthalmic Paediatr Genet. 1989; 10:293–298.17. Cassidy L, Taylor D. Congenital cataract and multisystem disorders. Eye (Lond). 1999; 13(Pt 3b):464–473.18. Sachdev N, Tiakumzuk S, Aulakh R, Brar GS. Anomalous bilateral lateral rectus muscles and anterior polar cataract with dysmorphic features. J AAPOS. 2009; 13:319–321.19. Melamed J, Eckert GU, Spadoni VS, et al. Ocular manifestations of congenital toxoplasmosis. Eye (Lond). 2010; 24:528–534.20. Sharan S, Sharma S, Billson FA. Congenital rubella cataract: a timely reminder in the new millennium? Clin Experiment Ophthalmol. 2006; 34:83–84.21. Chylack LT Jr, Wolfe JK, Singer DM, et al. The lens opacities classification system III: the Longitudinal Study of Cataract Study Group. Arch Ophthalmol. 1993; 111:831–836.22. Kim H, Joo CK. The prevalence and demographic characteristics of anterior polar cataract in a hospital-based study in Korea. Korean J Ophthalmol. 2008; 22:77–80.23. Kim HJ, Park JW, Joo CK. An epidemiological study of the risk factors associated with anterior polar cataract. J Korean Ophthalmol Soc. 2003; 44:606–614.24. Majima K, Majima Y. Histopathological and cell biological analyses of the formation mechanism of anterior polar cataract. Ophthalmologica. 1999; 213:34–39.25. Hess R, Woo G. Vision through cataracts. Invest Ophthalmol Vis Sci. 1978; 17:428–435.26. Cinotti AA. Evaluation of indications for cataract surgery. Ophthalmic Surg. 1979; 10:25–31.27. Jaffe NS. Glare and contrast: indications for cataract surgery. J Cataract Refract Surg. 1986; 12:372–375.28. Koch DD. Glare and contrast sensitivity testing in cataract patients. J Cataract Refract Surg. 1989; 15:158–164.29. Neumann AC, McCarty GR, Steedle TO, et al. The relationship between cataract type and glare disability as measured by the Miller-Nadler glare tester. J Cataract Refract Surg. 1988; 14:40–45.30. Stifter E, Sacu S, Benesch T, Weghaupt H. Impairment of visual acuity and reading performance and the relationship with cataract type and density. Invest Ophthalmol Vis Sci. 2005; 46:2071–2075.31. Stifter E, Sacu S, Weghaupt H. Functional vision with cataracts of different morphologies: comparative study. J Cataract Refract Surg. 2004; 30:1883–1891.32. McCarty CA, Mukesh BN, Fu CL, Taylor HR. The epidemiology of cataract in Australia. Am J Ophthalmol. 1999; 128:446–465.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk of Depression Associated with Common Chronic Eye Diseases: A Study Using the 8th Korea National Health and Nutrition Examination Survey (2019–2021)
- Association between Vitamin D and Allergic Disease and Cataract in Korean Adults
- Prevalence and Clinical Characteristics of Dyslipidemia in Koreans
- Age classification for tooth loss management in Korean adults
- Factors Associated with Awareness, Treatment, and Control Rate of Hypertension among Korean Young Adults Aged 30–49 Years
