Modified Retroperitoneal Access for Percutaneous Intervention after Pancreaticoduodenectomy
- Affiliations
-
- 1Department of Diagnostic Radiology, Tan Tock Seng Hospital, Singapore 308433, Singapore. druei@yahoo.com
- KMID: 1705457
- DOI: http://doi.org/10.3348/kjr.2013.14.3.446
Abstract
- Percutaneous access to the surgical bed after pancreaticoduodenectomy can be a challenge, due to the post-operative anatomy alteration. However, immediate complications, such as surgical bed abscess or suspected tumor recurrence, are often best accessed percutaneously, as open surgical or endoscopic approaches are often difficult, if not impossible. We, hereby, describe a safe approach that is highly replicable, in accessing the surgical bed for percutaneous intervention, following pancreaticoduodenectomy.
MeSH Terms
-
Abscess/radiography/therapy
Bile Duct Neoplasms/pathology/radiography
Biopsy/methods
Catheterization/*methods
Cholangiocarcinoma/pathology/radiography
Drainage/instrumentation/*methods
Humans
Male
Middle Aged
Neoplasm Recurrence, Local/pathology/radiography
Pancreatic Diseases/radiography/therapy
*Pancreaticoduodenectomy
Postoperative Complications/radiography/*therapy
Radiography, Interventional/methods
Retroperitoneal Space
Figure
-
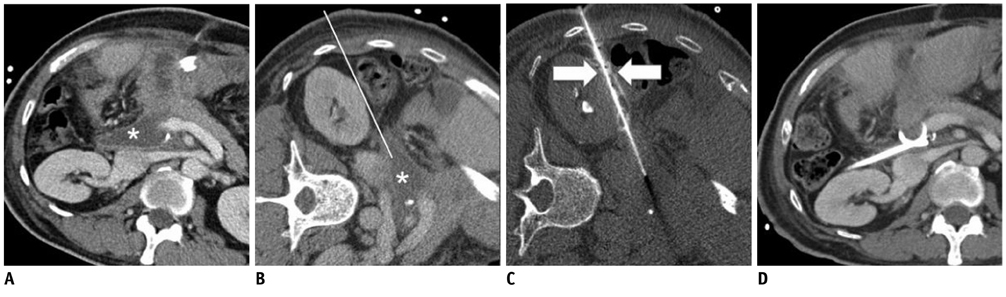
Fig. 1 Sixtyone year-old man with fever 7 days after pancreaticoduodenectomy. Contrast enhanced CT images (A) diagnostic (B) prior to drainage with patient in left decubitus position, shows abscess (*) in region of excised pancreatic head with overlying bowel loops and liver anteriorly. Planned trajectory in anterior pararenal space (white line) appeared narrow. (C) CT fluoroscopic image showing contrast-fluid hydrodissection (white arrows) widening space between right kidney and ascending colon to allow safe passage of needle. "Salinoma" was created by injecting contrast-fluid mixture continuously while advancing needle. (D) Contrast enhanced CT prior to drainage catheter removal, showing Cope loop of drainage catheter within surgical bed.
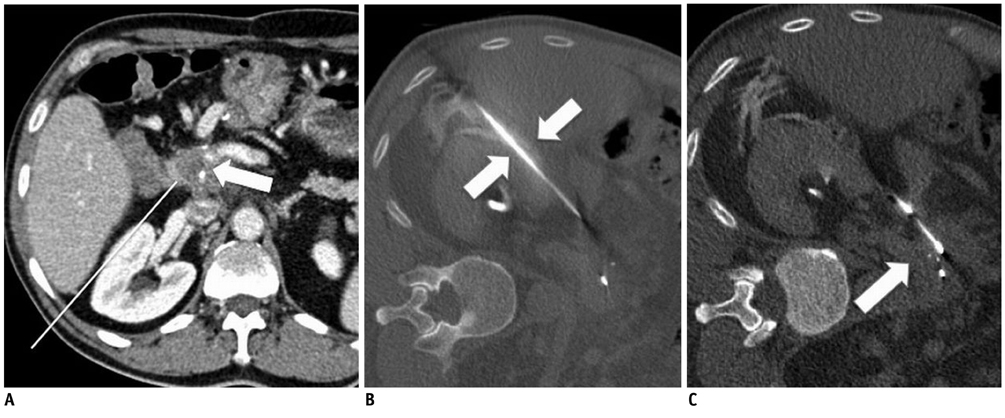
Fig. 2 Fiftyseven year-old man with suspicious lesion in surgical bed 3 years after pancreaticoduodenectomy. A. Contrast enhanced CT showed hypodense lesion in surgical bed, worrisome for tumor recurrence. Overlying bowel and vessels made anterior approach from biopsy unsuitable. Planned trajectory (white line) between segment VI of liver and right kidney is equivocal for needle passage without organ traversal. B. CT fluoroscopic image showing contrast-fluid hydrodissection (white arrows) used to create safe passage between liver and right kidney for guide needle. C. CT fluoroscopic image showing deployment of biopsy chamber into lesion (white arrow). Fine adjustments to biopsy location could be made by applying external torque on guide needle. Histology confirmed recurrent cholangiocarcinoma.
Reference
-
1. Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, et al. Six hundred fifty consecutive pancreaticoduodenectomies in the 1990s: pathology, complications, and outcomes. Ann Surg. 1997. 226:248–257. discussion 257-260.2. Gervais DA, Fernandez-del Castillo C, O'Neill MJ, Hahn PF, Mueller PR. Complications after pancreatoduodenectomy: imaging and imaging-guided interventional procedures. Radiographics. 2001. 21:673–690.3. Maher MM, Gervais DA, Kalra MK, Lucey B, Sahani DV, Arellano R, et al. The inaccessible or undrainable abscess: how to drain it. Radiographics. 2004. 24:717–735.4. Brandt KR, Charboneau JW, Stephens DH, Welch TJ, Goellner JR. CT- and US-guided biopsy of the pancreas. Radiology. 1993. 187:99–104.5. vanSonnenberg E, Wittich GR, Chon KS, D'Agostino HB, Casola G, Easter D, et al. Percutaneous radiologic drainage of pancreatic abscesses. AJR Am J Roentgenol. 1997. 168:979–984.6. Gupta S, Ahrar K, Morello FA Jr, Wallace MJ, Hicks ME. Masses in or around the pancreatic head: CT-guided coaxial fine-needle aspiration biopsy with a posterior transcaval approach. Radiology. 2002. 222:63–69.7. Sofocleous CT, Schubert J, Brown KT, Brody LA, Covey AM, Getrajdman GI. CT-guided transvenous or transcaval needle biopsy of pancreatic and peripancreatic lesions. J Vasc Interv Radiol. 2004. 15:1099–1104.8. DeBenedectis CM, Beland MD, Dupuy DE, Mayo-Smith WW. Utility of iodinated contrast medium in hydrodissection fluid when performing renal tumor ablation. J Vasc Interv Radiol. 2010. 21:745–747.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- RE: Percutaneous Retroperitoneal Access
- Obstructive Jaundice after Bilioenteric Anastomosis: Transhepatic and Direct Percutaneous Enteral Stent Insertion for Afferent Loop Occlusion
- Spontaneous Retroperitoneal Hemorrhage and Hemothorax After Intravenous Heparin Treatment
- Extra-anatomic percutaneous stenting of a malignant afferent loop obstruction following pancreaticoduodenectomy
- Percutaneous Enteral Stent Placement Using a Transhepatic Access for Palliation of Malignant Bowel Obstruction after Surgery
