J Korean Soc Spine Surg.
2005 Jun;12(2):140-145. 10.4184/jkss.2005.12.2.140.
Relationships between Posterior Ligament Complex Injury and Plain Radiograph in Thoracolumbar Spinal Fracture
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yonsei University, Wonju College of Medicine, Wonju, Korea.
- 2Department of Radiology, Yonsei University, Wonju College of Medicine, Wonju, Korea. par73@wonju.yonsei.ac.kr
- KMID: 1583457
- DOI: http://doi.org/10.4184/jkss.2005.12.2.140
Abstract
- STUDY DESIGN: A prospective study of 100 patients with thoracolumbar spinal fractures.
OBJECTIVES
To assess the relationships between a posterior ligament complex injury and plain radiograph in thoracolumbar spinal fractures. SUMMERY OF LITERATURE REVIEW: Some studies have reported the value of MRI for the evaluation of a posterior ligament complex injury. However, most of these did not evaluate the relationships between the posterior ligament complex and plain radiograph of the thoracolumbar spine fractures.
MATERIALS AND METHODS
100 patients with either a thoracolumbar compression or burst spinal fracture, from T11 to L2 levels, were evaluated by plain radiographs, taken in the supine position, and MRI taken within a week of the trauma. The wedge angle, Cobb's angle and anterior body height were measured on the plain radiographs, and the presence of posterior ligament complex injury on MRI was evaluated and analyzed.
RESULTS
In the compression fracture group, the wedge angle, Cobb's angle and anterior body height loss were 19.9+/-1.4 degrees, 14.3+/-2.2 degrees and 35.6+/-3.6%, respectively, in the posterior ligament complex injury subgroup, but only the anterior vertebral body height loss was statistically significant (p=0.04). In the burst fracture group, the wedge angle, Cobb's angle and anterior body height loss were 26.4+/-2.0 degrees, 23.3+/-1.7 degrees and 57.4+/-5.2%, respectively, in the posterior ligament complex injury subgroup, which were all statistically significant (p=0.00, 0.02, 0.00). With a sensitivity of 75% or greater, the wedge angle, Cobb's angle and anterior body height loss in compression and burst fractures were more than 15 degrees, 10 degrees and 30% and 20 degrees, 20 degrees and 40%, respectively.
CONCLUSIONS
When the values of wedge angle, Cobb's angle and anterior body height loss in the compression and burst fractures were more than 15 degrees, 10 degrees and 30% and 20 degrees, 20 degrees and 40%, respectively, and the sensitivity for the presence of a posterior ligament complex injury was more than 75%. Therefore, these values in the screening test are indicators for the presence of a posterior ligament complex injury. Further careful evaluations, such as MRI, are still required in deciding the appropriate treatment method.
Keyword
MeSH Terms
Figure
-
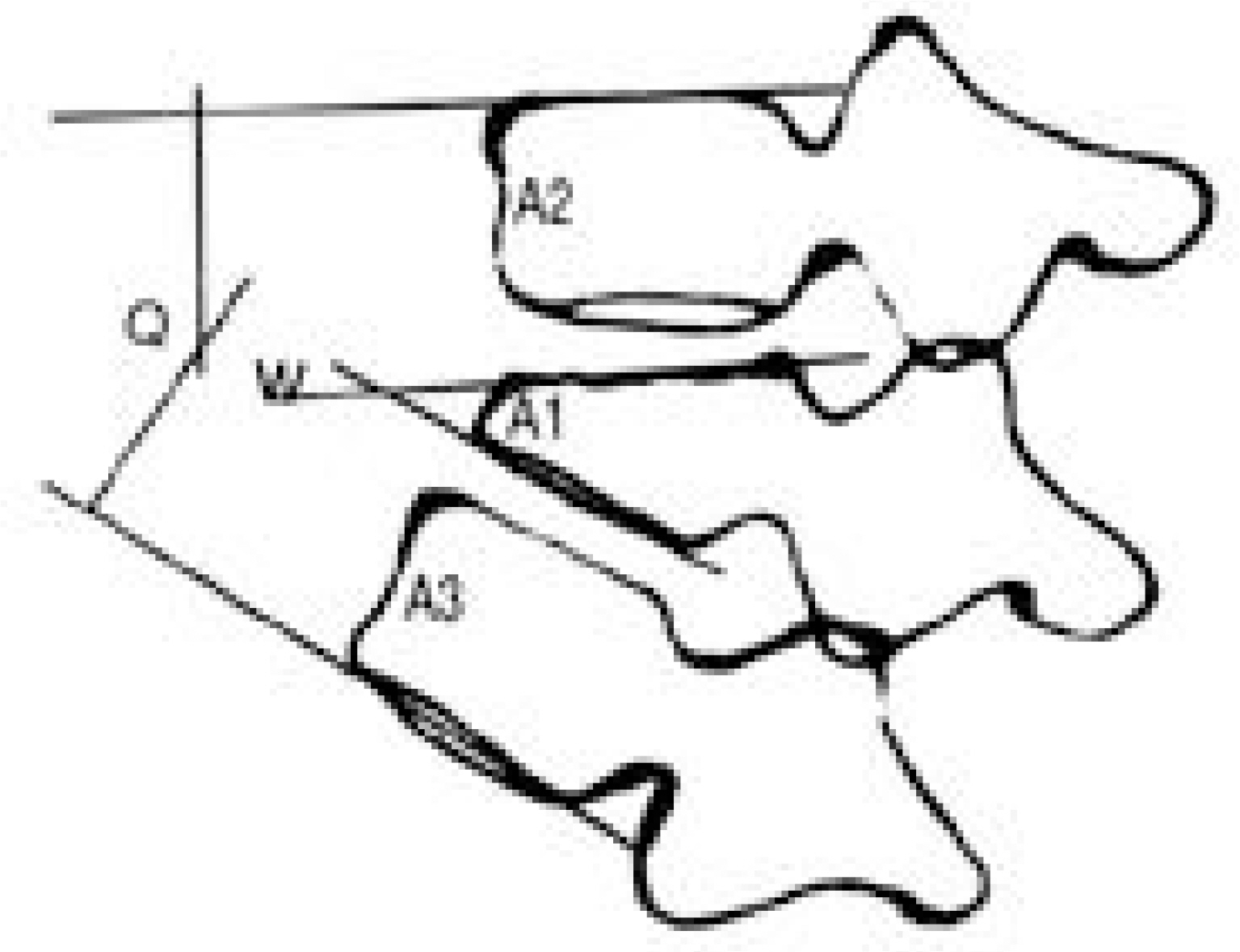
Fig. 1. Measurement of Cobb’s angle, Wedge angle and anterior body height. Q: Cobb’s angle, W: wedge angle, A: anterior body height, Compression of anterior body =(A2+A3)/2-A1× 100(A2+A3)/2

Fig. 2. State of the ligamentous structures observed on the MRI examinations. (A) No evidence of injury. (B) Edema in the inter-spinous space without evident discontinuity or elongation (C) Elongation of the interspinous space without discontinuity (D) Clear disruption of the posterior ligamentous complex
Reference
-
1). Benson DR, Burkus JK, Montesano PX, Sutherland TB, McLain RF. Unstable thoracolumbar and lumbar burst fractures treated with the AO fixateur interne. J Spinal Disord. 1992; 5:335–343.
Article2). Denis F, Amstrong GW, Searls K, Matta L. Acute thoracolumbar burst fractures in the absence of neurologic deficit: a comparison between operative and nonoperative treatment. Clin Orthop. 1984; 189:142–149.
Article3). Mumford J, Weinstein JN, Spratt KF, Goel VK. Thoracolumbar burst fractures: the clinical efficacy and outcome of nonoperative management. Spine. 1993; 18:955–970.4). Park HJ, Rah JH, Yoo KJ. Operative treatment of the thoracolumbar spine fractures with AO internal fixator. J Kor Spine Surg. 1996; 31:1116–1123.5). Reid DC, Hu R, Davis LA, Saboe LA. The nonoperative treatment of burst fractures of the thoracolumbar junction. J Trauma. 1988; 28:1188–1194.
Article6). Denis F. Spinal instability as defined by the three column spine concept in acute spinal trauma. Clin Orthop. 1984; 189:65–76.7). Shen WJ, Liu TJ, Shen YS. Nonoperative treatment versus posterior fixation for thoracolumbar junction burst fractures without neurological deficit. Spine. 2001; 26:1038–1045.8). Kropinger WJ, Frederickson BE, Mino DE, Yuan HA. Conservative treatment of fractures of the thoracic and lumbar spine. Othop Clin North Am. 1986; 17:161–170.9). Jacobs RR, Casey MP. Surgical management of thoracolumbar spinal fracture. Clin Orthop. 1984; 189:22–35.10). Terk MR, Hume-Neal M, Fraipont M, Ahmadi J, Colletti PM. Injury of the posterior ligament complex in patients with acute spinal trauma: evaluation by MR imaging. Am J Radiol. 1997; 168:1481–1486.
Article11). Kliewer MA, Gray L, Paver J, et al. Acute spinal ligament disruption: MR imaging with anatomic correlation. J Magn Reson Imaging. 1993; 3:855–861.
Article12). Oner FC, vd Rijt RH, Ramos LM, Groen GJ, Dhert WJ, Verbout AJ. Correlation of MR images of disc injuries with anatomic sections in experimental thoracolumbar fractures. Eur Spine J. 1999; 8:194–198.13). Denis F. The threee colum spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983; 8:817–831.14). Holdsworth FW. Fractures, dislocations, and fracture-dislocations of the spine. J Bone Joint Surg Br. 1963; 45:6–20.
Article15). McAfee PC, Yuan HA, Fredrickson BE, Lubicky JP. The value of computed tomography in thoracolumbar fractures. An analysis of 100 consecutive cases and a new classification. J Bone Joint Surg Am. 1983; 65:461–473.16). Saifuddin A, Noordeen H, Taylor BA, Bayley I. The role of imaging in the diagnosis and management of thoracolumbar burst fractures: current concepts and a review of the literature. Skeletal Radiol. 1996; 25:603–613.
Article17). Petersilge CA, Pathria MN, Emery SE, Masaryk TJ. Thoracolumbar burst fractures: Evaluation with MR imaging. Radiology. 1995; 194:49–54.
Article18). Lee HM, Kim HS, Kim DJ, Suk KS, Park JO, Kim NH. Reliability of magnetic resonance imaging in detecting posterior ligament complex injury in thoracolumbar spinal fractures. Spine. 2000; 25:2079–2084.
Article19). Abe E, Sato K, Shimada Y, Mizutani Y, Chiba M, Okuyama K. Thoracolumbar burst fracture with horizon -tal fracture of the posterior column. Spine. 1997; 22:83–87.20). Mehta JS, Reed MR, McVie JL, Sanderson PL. Weight-bearing radiograpghs in thoracolumbar fractures. Spine. 2004; 29:564–567.21). Ahn JS, Lee JK, Hwang DS, Kim YM, Kim WJ, Byun KH. The changes of kyphotic angle and anterior vertebral height after posterior or posterolateral fusion with transpedicular screws for thoracolumbar bursting fractures. J. Kor Trauma Asso. 1999; 12:379–387.22). Kim DJ, JM Wang. Burst fracture with distraction injury in the posterior column of the thoracolumbar spine. J Kor Spine Surg. 2001; 36:461–466.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationships between Radiological Change of Fractured Vertebrae and Posterior Ligament Complex Injury in Thoracolumbar Fracture
- Thoracolumbar Fracture with Posterior Ligament Complex Injury
- MRI Findings of Posterior Ligament Complex Injury in Thorcolumbar Bursting Fractures
- Injury of Posterior Ligament Complex with Cervical Spine Fracture
- Reliability of MRI to Detect Posterior Ligament Complex Injury in Thoracolumbar Spinal Fractures
