Clinical Role of F-18 FDG PET/CT in Squamous Cell Carcinoma of Head and Neck
- Affiliations
-
- 1Department of Nuclear Medicine, Hanyang University College of Medicine, Seoul, Korea. jtkim@hanyang.ac.kr
- 2Department of Nuclear Medicine, Armed Forces Daejeon Hospital, Daejeon, Korea.
- KMID: 1505104
- DOI: http://doi.org/10.7599/hmr.2009.29.3.274
Abstract
- Diagnostic imaging plays an important role in accurate staging, restaging, and treatment monitoring, and is essential in both planning adequate treatment and minimizing treatment-related toxicity and functional impairment in head and neck squamous cell carcinoma (HNSCC). MRI and CT remains the primary imaging modalities for the assessment of HNSCC, but F-18 FDG PET/CT had emerged as a vital adjunct when used in the appropriate clinical setting, such as: delineation of extent of regional lymph node involvement, detection of distant metastasis, identification of an unknown primary tumor, detection of an occasional synchronous primary tumor, monitoring of the treatment response, and long-term surveillance for recurrence and metastases. In this manuscript, clinical application of F-18 FDG PET/CT on HNSCC in initial staging, radiotherapy planning, carcinoma of unknown primary of squamous cell origin, evaluation of response to radiation and/or chemoradiation therapy, and prediction of prognosis will be discussed and other promising PET radiotracers will be introduced.
MeSH Terms
Figure
-
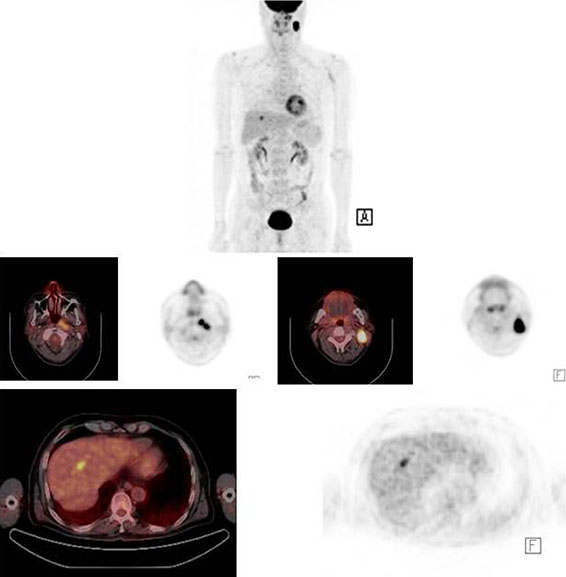
Fig. 1 Left nasopharyngeal cancer with left cervical lymphadenopathy. On PET/CT image there is another focal FDG uptake lesion in the liver, suggesting distant metastasis.
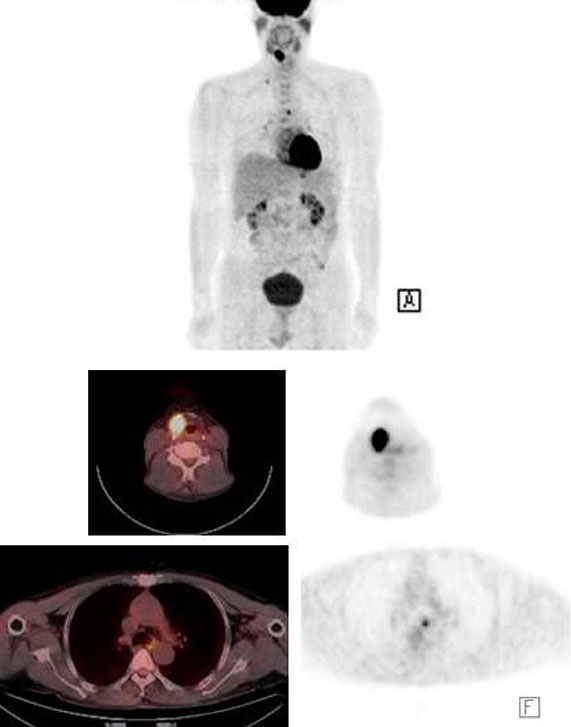
Fig. 2 Right vocal cord tumor with right supraclavicular lymph node metastasis. Another second primary malignancy is noted in esophagus.

Fig. 3 Metastatic squamous cell carcinoma of right cervical lymphadenopathy with unknown primary tumor. Focal FDG uptake was detected in right pyriform sinus on PET/CT, which was proven to be primary malignancy focus.

Fig. 4 False positive lymphadenopathy on FDG PET/CT in a patient with left vocal cord cancer, which was removed 10 days before. The patient didn't get treated, and followed FDG PET/CT one year later shows complete disappearance of hypermetabolic lesions.
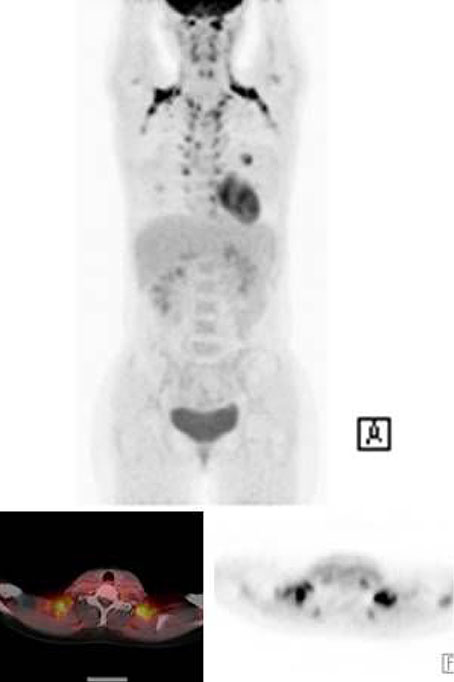
Fig. 5 Physiologic brown fat activity in bilateral neck should not be misinterpreted as pathologic cervical lymph nodes.
Reference
-
1. Kim JS, Lee JH. Clinical application of PET in head and neck cancer. Hanyang Med Rev. 2007; 27:16–22.2. Ha PK, Hdeib A, Goldenberg D, Jacene H, Patel P, Koch W, Califano J, Cummings CW, Flint PW, Wahl R, Tufano RP. The role of positron emission tomography and computed tomography fusion in the management of early-stage and advanced-stage primary head and neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg. 2006; 132:12–16.
Article3. Paulus P, Sambon A, Vivegnis D, Hustinx R, Moreau P, Collignon J, Deneufbourg JM, Rigo P. 18FDG-PET for the assessment of primary head and neck tumors: clinical, computed tomography, and histopathological correlation in 38 patients. Laryngoscope. 1998; 108:1578–1583.
Article4. Goerres GW, Schmid DT, Gratz KW, von Schulthess GK, Eyrich GK. Impact of whole body positron emission tomography on initial staging and therapy in patients with squamous cell carcinoma of the oral cavity. Oral Oncol. 2003; 39:547–551.
Article5. Schmid DT, Stoeckli SJ, Bandhauer F, Huguenin P, Shumid S, von Schlulthess GK, Goerres GW. Impact of positron emission tomography on the initial staging and therapy in locoregional advanced squamous cell carcinoma of the head and neck. Laryngoscope. 2003; 113:888–891.
Article6. Di Martino E, Nowak B, Hassan HA, Hausmann R, Adam G, Buell U, Westhofen M. Diagnosis and staging of head and neck cancer: a comparison of modern imaging modalities (positron emission tomography, computed tomography, color-coded duplex sonography) with panendoscopic and histopathologic findings. Arch Otolaryngol Head Neck Surg. 2000; 126:1457–1461.7. Schwartz DL, Rajendran J, Yueh B, Coltrera M, Anzai Y, Krohn K, Eary J. Staging of head and neck squamous cell cancer with extended-field FDG-PET. Arch Otolaryngol Head Neck Surg. 2003; 129:1173–1178.
Article8. Adams S, Baum RP, Stuckensen T, Bitter K, Hor G. Prospective comparison of 18F-FDG PET with conventional imaging modalities (CT, MRI, US) in lymph node staging of head and neck cancer. Eur J Nucl Med. 1998; 25:1255–1260.
Article9. Schoder H, Yeung HW. Positron emission imaging of head and neck cancer, including thyroid carcinoma. Semin Nucl Med. 2004; 34:180–197.
Article10. Dammann F, Horger M, Mueller-Berg M, Schlemmer H, Claussen CD, Hoffman J, Eschmann S, Bares R. Rational diagnosis of squamous cell carcinoma of the head and neck region: comparative evaluation of CT, MRI, and 18FDG PET. Am J Roentgenol. 2005; 184:1326–1331.
Article11. Yoon DY, Hwang HS, Chang SK, Rho YS, Ahn HY, Kim JH, Lee IJ. CT, MR, US, F-18 FDG PET/CT, and their combined use for the assessment of cervical lymph node metastasis in squamous cell carcinoma of the head and neck. Eur Radiol. 2009; 19:634–642.
Article12. Hyde NC, Prvulovich E, Newman L, Waddington WA, Visvikis D, Ell P. A new approach to pre-treatment assessment of the N0 neck in oral squamous cell carcinoma: the role of sentinel node biopsy and positron emission tomography. Oral Oncol. 2003; 39:350–360.
Article13. Stoeckli SJ, Steinert H, Pfaltz M, Schmid S. Is there a role for positron emission tomography with 18F-fluorodeoxyglucose in the initial staging of nodal negative oral and oropharyngeal squamous cell carcinoma. Head Neck. 2002; 24:345–349.
Article14. Schoder H, Carlson DL, Kraus DH, Stambuk HE, Gonen M, Erdi YE, Yeung HW, Huvos AG, Shah JP, Larson SM, Wong RJ. 18F-FDG PET/CT for detecting nodal metastases in patients with oral cancer staged N0 by clinical examination and CT/MRI. J Nucl Med. 2006; 47:755–762.15. Goyal P, Hsu JM, Kellman RM. Effect of F-18 FDG PET on the management of patients with head and neck squamous cell carcinoma. J Otolaryngol Head Neck Surg. 2008; 37:694–699.16. Wax MK, Myers LL, Gabalski EC, Husain S, Gona JM, Nabi H. Positron emission tomography in the evaluation of synchronous lung lesions in patients with untreated head and neck cancer. Arch Otolaryngol Head Neck Surg. 2002; 128:703–707.
Article17. Keyes JW Jr, Chen MY, Watson NE Jr, Greven KM, McGuirt WF, Williams DW III. FDG PET evaluation of head and neck cancer: value of imaging the thorax. Head Neck. 2000; 22:105–110.
Article18. Perlow A, Bui C, Shreve P, Sundgren PC, Teknos TN, Mukherji SK. High incidence of chest malignancy detected by FDG PET in patients suspected of recurrent squamous cell carcinoma of the upper aerodigestive tract. J Comput Assist Tomogr. 2004; 28:704–709.
Article19. Regelink G, Brouwer J, de Bree R, Pruim J, van der Laan BF, Vaalburg W, Hoekstra OS, Comans EF, Vissink A, Leemans CR, Roodenburg JL. Detection of unkown primary tumours and distant metastases in patients with cervical metastases: value of FDG PET versus conventional modalities. Eur J Nucl Med Mol Imaging. 2002; 29:1024–1030.
Article20. Nieder C, Gregoire V, Ang KK. Cervical lymph node metastases from occult squamous cell carcinoma: cut down a tree to get an apple? Int J Radiat Oncol Biol Phys. 2001; 50:727–733.
Article21. Jungehulsing M, Scheidhauer K, Damm M, Pietrzyk U, Eckel H, Schicha H, Sennert E. FDG PET is a sensitive tool for the detection of occult primary cancer (carcinoma of unknown primary syndrome) with head and neck lymph node manifestation. Otolaryngol Head Neck Surg. 2000; 123:294–301.
Article22. Bohuslavizki KH, Klutmann S, Kroger S, Sonnermann U, Buchert R, Werner JA, Meser J, Clausen M. FDG PET detection of unknown primary tumors. J Nucl Med. 2000; 41:816–822.23. Stokkel MP, Terhaard CH, Hordijk GJ, van Rijk PP. The detection of unknown primary tumors in patients with cervical metastases by dual-head positron emission tomography. Oral Oncol. 1999; 35:390–394.
Article24. Lassen U, Daugaard G, Eigtved A, Damgaard K, Friberg L. F-18 FDG whole body positron emission tomography (PET) in patients with unknown primary tumors (UTP). Eur J Cancer. 1999; 35:1076–1082.
Article25. Greven KM, Keye JW Jr, William DW 3rd, Watson N. Occult primary tumors of the head and neck: lack of benefit from positron emission tomography imaging with FDG. Cancer. 1999; 86:114–118.26. Braams JW, Pruim J, Kole AC, Nikkels PG, Vaalburg W, Vermey A, Roodenburg JL. Detection of unknown primary head and neck tumors by positron emission tomography. Int J Oral Maxillofac Surg. 1997; 26:112–115.
Article27. Paul SA, Stoeckli SJ, von Schulthess GK, Goerres GW. FDG PET and PET/CT for detection of the primary tumor in patients with cervical nonsquamous cell carcinoma metastasis of an unknown primary. Eur Arch Otorhinolaryngol. 2007; 264:189–195.
Article28. Freudenberg LS, Fischer M, Antoch G, Jentzen W, Gutzeit A, Rosenbaum SJ, Bockisch A, Egelhof T. Dual modality of FDG PET/CT in patients with cervical carcinoma of unknown primary. Med Princ Pract. 2005; 14:155–160.
Article29. Yao M, Smith RB, Graham MM, Hoffman HT, Tan H, Funk GF, Graham SM, Chang K, Dornfeld KJ, Menda Y, Buatti JM. The role of FDG PET in management of neck metastasis from head-and-neck cancer after definitive radiation treatment. Int J Radiat Oncol Biol Phys. 2005; 63:991–999.
Article30. Ong SC, Schoder H, Lee NY, Patel SG, Carlson D, Fury M, Pfister DG, Shah JP, Larson SM, Kraus DH. Clinical utility of FDG PET/CT in assessing the neck after concurrent chemoradiotherapy for locoregional advanced head and neck cancer. J Nucl Med. 2008; 49:532–540.
Article31. Lonneux M, Lawson G, Ide C, Bausart R, Remacle M, Pauwels S. Positron emission tomography with FDG for suspected head and neck tumor recurrence in the symptomatic patient. Laryngoscope. 2000; 110:1493–1497.
Article32. Andrade RS, Heron DE, Degirmenci B, Filho PA, Branstetter BF, Seethala RR, Ferris RL, Avril N. Posttreatment assessment of response using FDG PET/CT for patients treated with definitive radiation therapy for head and neck cancers. Int J Radiat Oncol Biol Phys. 2006; 65:1315–1322.
Article33. Greven KM, Williams DW III, McGuirt WF Sr, D'Agostino RB Jr. Serial positron emission tomography scans following radiation therapy of patients with head and neck cancer. Head Neck. 2001; 23:942–946.
Article34. Ciernik IF, Dizendorf E, Baumert BG, Reiner B, Burger C, Davis JB, Lutolf UM, Steinert HC, Von Schulthess GK. Radiation treatment planning with an integrated positron emission and computer tomography (PET/CT): a feasibility study. Int J Radiat Oncol Biol Phys. 2003; 57:853–863.
Article35. Heron DE, Andrade RS, Flickinger J, Johnson J, Agarwala SS, Wu A, Kalnicki S, Avril N. Hybrid PET-CT simulation for radiation treatment planning in head-and-neck cancers: a brief technical report. Int J Radiat Oncol Biol Phys. 2004; 60:1419–1424.
Article36. Torizuka T, Tanizaki Y, Kanno T, Futatsubashi M, Naitou K, Ueda Y, Ouchi Y. Prognostic value of 18F-FDG PET in patients with head and neck squamous cell cancer. AJR Am J Roentgenol. 2009; 192:W156–W160.37. Machtay M, Natwa M, Andrel J, Hyslop T, Anne PR, Lavarino J, Intenzo CM, Keane W. Pretreatment FDG PET standardized uptake value as a prognostic factor for outcome in head and neck cancer. Head Neck. 2009; 31:195–201.
Article38. Liao CT, Chang JT, Wang HM, Ng SH, Hsueh C, Lee LY, Lin CH, Chen IH, Hwang SF, Cheng AJ, Yen TC. Preoperative [18F]fluorodeoxyglucose positron emission tomography standardized uptake value of neck lymph nodes predicts neck cancer control and survival rates in patients with oral cavity squamous cell carcinoma and pathologically positive lymph nodes. Int J Radiat Oncol Biol Phys. 26. 12. 2008; [Epub ahead of print].
Article39. Suzuki H, Hasegawa Y, Terada A, Hyodo I, Nakashima T, Nishio M, Tamaki T. FDG-PET predicts survival and distant metastasis in oral squamous cell carcinoma. 18. 09. 2008; [Epub ahead of print].
Article40. Rasey JS, Grierson JR, Wiens LW, Kolb PD, Schwatz JL. Validation of FLT uptake as a measure of thymidine kinase-I activity in A549 carcinoma cells. J Nucl Med. 2002; 43:1210–1217.41. Schwartz JL, Tamura Y, Jordan R, Grierson JR, Krohn KA. Effect of p53 activation on cell growth, thymidine kinase-1 activity, and 3'-deoxy-3'fluorothymidine uptake. Nucl Med Biol. 2004; 31:419–423.
Article42. Nordsmark M, Bentzen SM, Rudat V, Brizel D, Lartigau E, Stadler P, Becker A, Adam M, Molls M, Dunst J, Terris DJ, Overgaard J. Prognostic value of tumor oxygenation in 397 head and neck tumors after primary radiation therapy: an international multicenter study. Radiother Oncol. 2005; 77:18–24.
Article43. Rischin D, Hicks RJ, Fisher R, Binns D, Corry J, Porceddu S, Peters LJ. Trans-Tasman Radiation Oncology Group Study 98.02. Prognostic significance of [18F]-misonidazole positron emission tomography-detected tumor hypoxia in patients with advanced head and neck cancer randomly assigned to chemoradiation with or without tirapazamine: a substudy of Trans-Tasman Radiation Oncology Group Study 98.02. J Clin Oncol. 2006; 24:2098–2104.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Application of PET in Head and Neck Cancer
- The Role of 18F-FDG PET/CT for Evaluation of Cervical Metastatic Lymph Nodes in a Patient with Metallic Artifacts from Dental Prosthesis: a Case Report
- Accuracy of F-18 FDG PET/CT in Preoperative Assessment of Cervical Lymph Nodes in Head and Neck Squamous Cell Cancer: Comparison with CT/MRI
- (18)F-FDG PET/CT in Patients with Initially Diagnosed Adenoid Cystic Carcinoma of the Head and Neck: Clinicoplathologic Correlation
- A Case of Synchronous Triple Primary Cancer Undetected by the PET-CT
