A Case of Cryptogenic Stroke Associated with Patent Foramen Ovale Coexisting with Pulmonary Embolisms, Deep Vein Thromboses, and Renal Artery Infarctions
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Presbyterian Medical Center, Jeonju, Korea. jppark74@gmail.com
- KMID: 1491103
- DOI: http://doi.org/10.4070/kcj.2012.42.12.853
Abstract
- A paradoxical embolism is defined as a systemic arterial embolism requiring the passage of a venous thrombus into the arterial circulatory system through a right-to-left shunt, and is commonly related to patent foramen ovale (PFO). However, coexisting pulmonary embolisms, deep vein thromboses (DVT), and multipe systemic arterial embolisms, associated with PFO, are rare. Here, we report a patient who had a cryptogenic ischemic stroke, associated with PFO, which is complicated with a massive pulmonary thromboembolism, DVT, and renal infarctions, and subsequently, the patient was treated using a thrombolytic therapy.
Keyword
MeSH Terms
Figure
-

Fig. 1 Brain MRI and MRA. A: brain MRI reveals a high signal intensity lesion in the right middle cerebral artery in the diffusion image (arrow). B: MRA shows total occlusion of genu of the right middle cerebral artery (arrow). MRA: magnetic resonance angiogram.
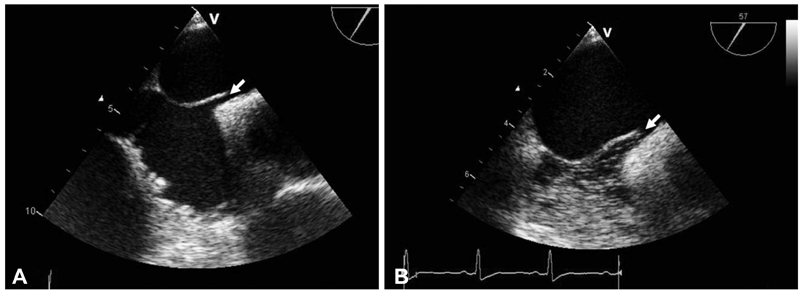
Fig. 2 TEE and TEE with agitated saline test. A: TEE shows a separation of the septum primum from septum secundum that constitutes a PFO (arrow). B: agitated saline injection test identified a right-to-left microbubble shunting during a Valsalva maneuver (arrow). TEE: transesophageal echocardiogram, PFO: patent foramen ovale.

Fig. 3 Chest CT angiogram. A: chest CT shows pulmonary embolism of the right inferior pulmonary artery and left pulmonary segmental artery (arrows). B: 9 hours after thrombolytic therapy, the follow-up CT angiogram shows resolved state of pulmonary embolism (arrows). CT: computed tomography.

Fig. 4 CT angiogram after thrombolytic therapy. A and B: CT venogram of the pelvis and lower extremities show thrombi in the left common iliac vein (A, arrow) and multiple thrombi in both peroneal veins (B, arrows). C: abdomen CT reveals newly developed multiple wedge-shaped hypoperfusion lesions in both kidneys, compatible with renal infarctions (arrows). CT: computed tomography.
Cited by 1 articles
-
Post-Operative Multiple Thrombosis Associated with Patent Foramen Ovale: Embolic Stroke, Right Atrial Thrombi, Pulmonary Embolism and Deep Vein Thrombosis
Sun-Young Cho, Ho-Joong Youn, Mi-Youn Park, Byung-Ju Shim, Seung-Jae Lee, Jeong-Ho Kim, Jung-Ku Park, Chang-Yul Oh, So-Hyun Ahn, Woo-Hyun Cho
J Cardiovasc Ultrasound. 2015;23(3):177-180. doi: 10.4250/jcu.2015.23.3.177.
Reference
-
1. Webster MW, Chancellor AM, Smith HJ, et al. Patent foramen ovale in young stroke patients. Lancet. 1988. 2:11–12.2. Lechat P, Mas JL, Lascault G, et al. Prevalence of patent foramen ovale in patients with stroke. N Engl J Med. 1988. 318:1148–1152.3. Oh BH, Park SW, Choi YJ, et al. Prevalence of the patent foramen ovale in young patients with ischemic cerebrovascular disease: transesophageal contrast echocardiographic study. Korean Circ J. 1993. 23:217–222.4. Clergeau MR, Hamon M, Morello R, Saloux E, Viader F, Hamon M. Silent cerebral infarcts in patients with pulmonary embolism and a patent foramen ovale: a prospective diffusion-weighted MRI study. Stroke. 2009. 40:3758–3762.5. Pelletier M, Bugeaud R, Ibrahim R, Morency G, Kouz S. Successful thrombolysis of a stroke with a pulmonary embolism in a young woman. J Emerg Med. 2010. 39:443–448.6. Cramer SC, Rordorf G, Maki JH, et al. Increased pelvic vein thrombi in cryptogenic stroke: results of the Paradoxical Emboli from Large Veins in Ischemic Stroke (PELVIS) Study. Stroke. 2004. 35:46–50.7. Lim DS, Jeong ES, Jung JS, et al. A case of paradoxical renal embolism through patent foramen ovale. Korean J Nephrol. 2011. 30:667–670.8. Caretta G, Robba D, Bonadei I, et al. Multiorgan paradoxical embolism consequent to acute pulmonary thromboembolism with patent foramen ovale: a case report. Cases J. 2009. 2:8358.9. Kouskov OS, Nichols DJ, O'Hearn DJ. Paradoxical arterial embolism involving both upper extremities in a patient with pulmonary embolism and a patent foramen ovale. Clin Appl Thromb Hemost. 2011. 17:E98–E101.10. Tanislav C, Puille M, Pabst W, et al. High frequency of silent pulmonary embolism in patients with cryptogenic stroke and patent foramen ovale. Stroke. 2011. 42:822–824.11. Thomas DV, Bynevelt M, Price R. Paradoxical embolization via a patent foramen ovale following acute pulmonary embolism. Australas Radiol. 2005. 49:501–504.12. Augustinos P, Ouriel K. Invasive approaches to treatment of venous thromboembolism. Circulation. 2004. 110:9 Suppl 1. I27–I34.13. Guo S, Roberts I, Missri J. Paradoxical embolism, deep vein thrombosis, pulmonary embolism in a patient with patent foramen ovale: a case report. J Med Case Rep. 2007. 1:104.14. Dao CN, Tobis JM. PFO and paradoxical embolism producing events other than stroke. Catheter Cardiovasc Interv. 2011. 77:903–909.15. Konstantinides S, Geibel A, Kasper W, Olschewski M, Blümel L, Just H. Patent foramen ovale is an important predictor of adverse outcome in patients with major pulmonary embolism. Circulation. 1998. 97:1946–1951.16. Khairy P, O'Donnell CP, Landzberg MJ. Transcatheter closure versus medical therapy of patent foramen ovale and presumed paradoxical thromboemboli: a systematic review. Ann Intern Med. 2003. 139:753–760.17. Windecker S, Wahl A, Nedeltchev K, et al. Comparison of medical treatment with percutaneous closure of patent foramen ovale in patients with cryptogenic stroke. J Am Coll Cardiol. 2004. 44:750–758.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Post-Operative Multiple Thrombosis Associated with Patent Foramen Ovale: Embolic Stroke, Right Atrial Thrombi, Pulmonary Embolism and Deep Vein Thrombosis
- A Case of Paradoxical Renal Embolism through Patent Foramen Ovale
- Patent Foramen Ovale and Cryptogenic Stroke
- A Case of Bilateral Posterior Cerebral Artery Infarction with Patent Foramen Ovale
- Posterior Cerebral Artery Infarction in a Patient with Coexisting Hereditary Hemorrhagic Telangiectasia and Patent Foramen Ovale
