Recurrent Catecholamine-Induced Cardiomyopathy in a Patient With a Pheochromocytoma
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyungpook National University Medical School, Daegu, Korea. ddhyang@knu.ac.kr
- KMID: 1490702
- DOI: http://doi.org/10.4070/kcj.2009.39.6.254
Abstract
- Pheochromocytomas presents with variable clinical manifestations. Cardiomyopathy caused by a pheochromocytoma is well known. We report the case of a 62-year-old woman with recurrent left ventricular dysfunction, who was subsequently found to have a pheochromocytoma. The patient had two different patterns of cardiomyopathy. Patients with a cardiomyopathy, of non-specific origin, should have a pheochromocytoma ruled out.
Keyword
MeSH Terms
Figure
-

Fig. 1 Echocardiography showing akinesis of the basal and mid-ventricular segments, with preserved contractility of the apical segments. A: apical 4 chamber view of end-diastole (Left) and end-systole (Right). B: apical 2 chamber view of end-diastole (Left) and end-systole (Right).
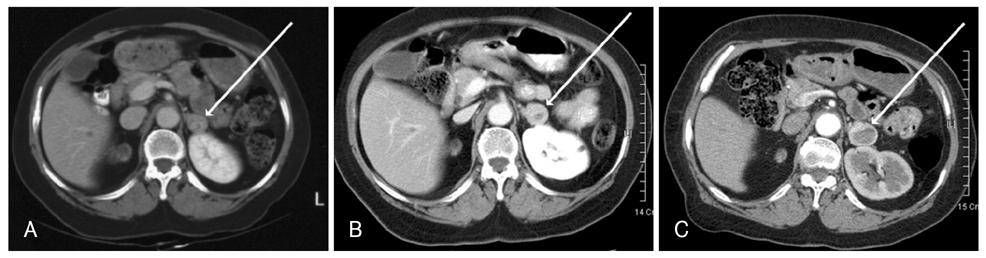
Fig. 2 An enhanced abdominal computed tomographic scan. A: November. 14, 2000-2 cm left adrenal mass with central low density lesion (arrow). B: March 8, 2002-the left adrenal mass increased to 2.5 cm (arrow). C: September 3, 2004-The size of left adrenal mass was about 3 cm (arrow).
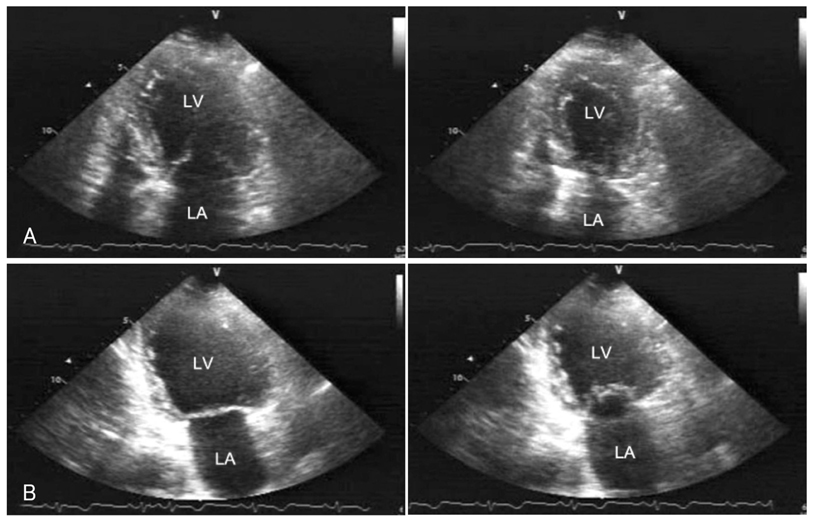
Fig. 3 Echocardiography performed in December of 2003 showing decreased motion of the apical and mid-segments, with preserved contractility of the basal segments. A: apical 4 chamber view of end-diastole (Left) and end-systole (Right). B: apical 2 chamber view of end-diastole (Left) and end-systole (Right). LA: left atrium, LV: left ventricular.
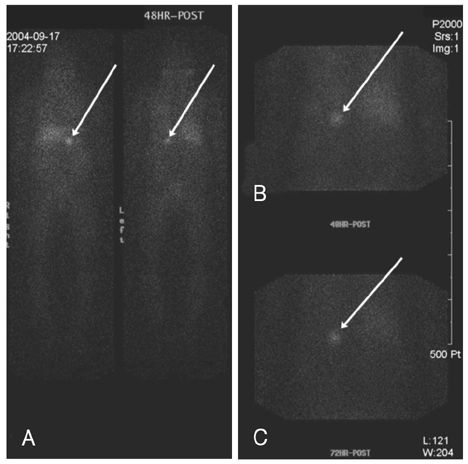
Fig. 4 I-131 MIBG scan performed 48 hours after isotope injection, shows increased tracer uptake in the left adrenal gland (arrow), and normal tracer activity in the liver and gastrointestinal tract (A and B). I-131 MIBG scan performed 72 hours after isotope injection, also shows increased uptake in the left adrenal gland (arrow, C). MIBG: metaiodobenzylguanidine.
Reference
-
1. Mann DL, Kent RL, Parsons B, Cooper G 4th. Adrenergic effects on the biology of the adult mammalian cardiocyte. Circulation. 1992. 85:790–804.2. Szakacs JE, Cannon A. L-Norepinephrine myocarditis. Am J Clin Pathol. 1958. 30:425–434.3. Sardesai SH, Mourant AJ, Sivathandon Y, Farrow R, Gibbons DO. Phaeochromocytoma and catecholamine induced cardiomyopathy presenting as heart failure. Br Heart J. 1990. 63:234–237.4. Attar MN, Moulik PK, Salem GD, Rose EL, Khaleeli AA. Phaeochromocytoma presenting as dilated cardiomyopathy. Int J Clin Pract. 2003. 57:547–548.5. Hong SK, Choi H, Lee SC. Reversal of dilated cardiomyopathy with medical therapy in a case of pheochromocytoma. Korean Circ J. 1998. 28:284–290.6. Takizawa M, Kobayakawa N, Uozumi H, et al. A case of transient left ventricular ballooning with pheochromocytoma, supporting pathogenetic role of catecholamines in stress-induced cardiomyopathy or takotsubo cardiomyopathy. Int J Cardiol. 2007. 114:e15–e17.7. Takeno Y, Eno S, Hondo T, Matsuda K, Zushi N. Pheochromocytoma with reversal of tako-tsubo-like transient left ventricular dysfunction: a case report. J Cardiol. 2004. 43:281–287.8. Sanchez-Recalde A, Costero O, Oliver JM, Iborra C, Ruiz E, Sobrino JA. Images in cardiovascular medicine: pheochromocytoma-related cardiomyopathy: inverted Takotsubo contractile pattern. Circulation. 2006. 113:e738–e739.9. van de Walle SO, Gevaert SA, Gheeraert PJ, De Pauw M, Gillebert TC. Transient stress-induced cardiomyopathy with an "inverted takotsubo" contractile pattern. Mayo Clin Proc. 2006. 81:1499–1502.10. Copetti R, Gonano C, Colombo T, Cattarossi L. "Inverted Takotsubo" pattern. Resuscitation. 2007. 74:394.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Catastrophic catecholamine-induced cardiomyopathy rescued by extracorporeal membrane oxygenation in recurrent malignant pheochromocytoma
- A case of pheochromocytoma with acute pancreatitis and catecholamine-induced cardiomyopathy
- Anesthetic experience of pheochromocytoma resection with catecholamine-induced cardiomyopathy and congestive heart failure : A case report
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
- A Case of Reversible Catecholamine Induced Cardiomyopathy by Retrobulbar Epinephrine Injection
