Histopathologic Analysis of BI-RADS Category 4a Breast Lesions Diagnosed by Ultrasonography
- Affiliations
-
- 1Breast Center, MizMedi Hospital, Seoul, Korea. drjo514@yahoo.co.kr
- 2Department of General Surgery, MizMedi Hospital, Seoul, Korea.
- 3Department of Diagnostic Radiology, MizMedi Hospital, Seoul, Korea.
- 4Department of Pathology, MizMedi Hospital, Seoul, Korea.
- 5Department of Pathology, National Health Insurance Corporation Ilsan Hospital, Goyang, Korea.
- KMID: 1485107
- DOI: http://doi.org/10.4048/jbc.2008.11.3.139
Abstract
- PURPOSE
We analyzed the histopathologic findings of the patients with ultrasongraphic Breast Imaging Reporting and Data System (BI-RADS) Category 4a breast lesions to determine which patient can be excluded from any invasive, diagnostic procedure in the future. METHODS: Of the 180 cases of BI-RADS Category 4a breast lesions that were diagnosed with ultrasonography during a 6 month-period, 132 cases were pathologically confirmed and these were analyzed retrospectively. Four benign cases that did not undergo any further procedure after fine needle biopsy and 6 malignant cases (4.5%) were excluded from this study. RESULTS: Of the 122 cases, 77 cases (63.1%) showed homogeneous benign finding, and 45 cases (36.9%) showed heterogeneous finding that was made up of two or more different pathologic lesions. Fibroadenoma (55.8%) was the most frequent pathologic finding in the cases with homogeneous finding, followed by fibrocystic change (14.3%), and fibrosis (7.8%). The cases with heterogeneous finding presented fibrocystic change (55.5%), microcalcification (48.8%), ductal hyperplasia (42.2%), and fibroadenoma (31.1%) in the order of frequency. CONCLUSION: Lesion with heterogeneous histopathologic nature was the most frequent finding defined as category 4a in breast ultrasonography, followed by fibrodenoma, fibrocystic change, microcalcification, and ductal hyperplasia. Refining more specific ultrasonographic findings of these lesions would guarantee that radiologists exclude more benign lesions from category 4a.
Keyword
MeSH Terms
Figure
-

Fig 1 Fibroadenoma categorized as Category 4a. (A) The mass shows heterogeneous and low internal echo and it has microlobulated and angular margin. But its axis is parallel and it has posterior enhancement without peripheral thickening. The picture was scanned with ATL HDI 5000, Phillips, USA. (B) The picture was taken from the above lesion. Its stromal component shows marked fibrosis and lack of cellularity. (C) Cystically dilated ducts and tubular glands are seen in loose mixoid stroma (H&E, ×100).
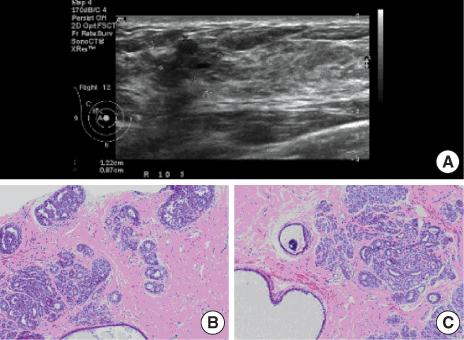
Fig 2 Heterogeneous lesion defined as Category 4a. (A) The mass shows heterogeneous and low internal echo and it has microlobulated margin. It also has posterior acoustic shadowing in part. There is no secondary sign on the surrounding tissue, like architectural distortion, Cooper's ligament thickening or cutoff, peripheral thickening. The picture was scanned with ATL HDI 5000, Phillips, USA. (B) Several foci of ductal hyperplasia are seen on the top. Fibrocystic change is also seen on the bottom. (C) Microcalcification is in the dilated duct on the left of a large component of adenosis (H&E, ×100).
Reference
-
1. Kerlikowske K, Grady D, Barclay J, Sickles EA, Ernster V. Effect of age, breast density, and family history on the sensitivity of first screening mammography. JAMA. 1996. 276:33–38.
Article2. Lee HD, Park HB, Koo JY, Oh SM, Lim JY, Cha KH, et al. Study for M-mammographic patterns of Korean breast cancer. J Korean Breast Cancer. 1999. 2:86–94.3. Kopans D, D'Orsi C. ACR system enhances mammography reporting. Diagn Imaging (San Franc). 1992. 14:125–132.4. American College of Radiology. Breast imaging and reporting system-ultrasound (BI-RADS®). 2003. 4th ed. Reston: American College of Radiology.5. Demsey PJ. The importance of resolution in the clinical application of breast sonography. Ultrasound Med Biol. 1988. 14:43–48.
Article6. Jackson VP. The role of US in breast imaging. Radiology. 1990. 177:305–311.
Article7. Stavros AT, Thickman D, Rapp CL, Dennis MA, Parker SH, Sisney GA. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995. 196:123–134.
Article8. American College of Radiology. Practice guideline for the performance of the breast ultrasound examination. 2002. Reston: Americal College of Radiology.9. Flobbe K, Bosch AM, Kessels AG, Beets GL, Nelemans PJ, von Meyenfeldt MF, et al. The additional diagnostic value of ultrasonography in the diagnosis of breast cancer. Arch Intern Med. 2003. 163:1194–1199.
Article10. Berg WA, Campassi CI, Ioffe OB. Cystic lesions of the breast: sonographic-pathologic correlation. Radiology. 2003. 227:183–191.
Article11. Hong AS, Rosen EL, Soo MS, Baker JA. BI-RADS for sonography: positive and negative predictive values of sonographic features. Am J Roentgenol. 2005. 184:1260–1265.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes of US BI-RADS 4A, 4B, and 4C Lesions
- Usefulness of ultrasound elastography in reducing the number of Breast Imaging Reporting and Data System category 3 lesions on ultrasonography
- Categorization and Evaluation of Usefulness of Breast Lesions with using Ultrasound BI-RADS (Breast Imaging Reporting and Data system)
- Predictive Value of BI-RADS Category 4A and 4B Lesions Detected on Breast Ultrasonography: Single Center Experience
- Synchronous BI-RADS Category 3 Lesions on Preoperative Ultrasonography in Patients with Breast Cancer: Is Short-Term Follow-Up Appropriate?
