Tuberc Respir Dis.
2008 Jan;64(1):39-43. 10.4046/trd.2008.64.1.39.
A Case of Persistent Hiccup in a Patient with Non-small Cell Lung Cancer
- Affiliations
-
- 1Department of Internal Medicine, School of Medicine, Ewha Womans University, Seoul, Korea. greenzone@ewha.ac.kr
- 2Department of Pathology, School of Medicine, Ewha Womans University, Seoul, Korea.
- KMID: 1478140
- DOI: http://doi.org/10.4046/trd.2008.64.1.39
Abstract
- A hiccup is caused by involuntary, intermittent, and spasmodic contractions of the diaphragm and intercostal muscles. It starts with a sudden inspiration and ends with an abrupt closure of the glottis. Even though a hiccup is thought to develop through the hiccup reflex arc, its exact pathophysiology is still unclear. The etiologies include gastrointestinal disorders, respiratory abnormalities, psychogenic factors, toxic-metabolic disorders, central nervous system dysfunctions and irritation of the vagus and phrenic nerves. Most benign hiccups can be controlled by traditional empirical therapy such as breath holding and swallowing water. However, though rare, a persistent hiccup longer than 48 hours can lead to significant adverse effects including malnutrition, dehydration, insomnia, electrolyte imbalance, and cardiac arrhythmia. An intractable hiccup can sometimes even cause death. We herein describe a patient with non-small cell lung cancer who was severely distressed by a persistent hiccup.
Keyword
MeSH Terms
Figure
-

Figure 1 Chest X-ray on admission shows a large amount of pleural effusion in the left hemithorax.
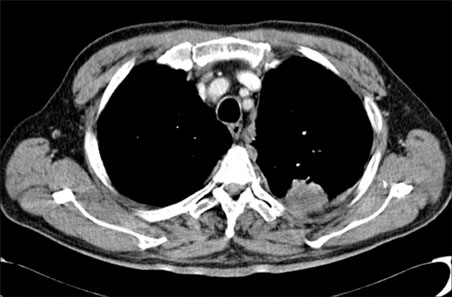
Figure 2 Chest CT scan reveals pleural nodularity and an irregular-shaped subpleural mass in the left upper lobe.

Figure 3 Chest CT scan shows multiple enlarged lymph nodes in the left hilum and both paratracheal areas.

Figure 4 Histopathologic findings reveal poorly differentiated adenocarcinoma (A: H&E stain, ×100, B: H&E stain, ×400).
Reference
-
1. Alonso-Navarro H, Rubio L, Jimenez-Jimenez FJ. Refractory hiccup: successful treatment with gabapentin. Clin Neuropharmacol. 2007. 30:186–187.2. Kahrilas PJ, Shi G. Why do we hiccup? Gut. 1997. 41:712–713.3. Choi GW, Kwak KH, Jeon YH, Hong JG. Treatment of postoperative intractable hiccup patient with unilateral phrenic nerve block: a case report. Korean J Anesthesiol. 2006. 50:592–595.4. Smith HS, Busracamwongs A. Management of hiccups in the palliative care population. Am J Hosp Palliat Care. 2003. 20:149–154.5. Pollack MJ. Intractable hiccups: a serious sign of underlying systemic disease. J Clin Gastroenterol. 2003. 37:272–273.6. Lim BS, Choi WY, Choi JW, Shin DH, Park SS, Lee JH. A case of steroid induced intractable hiccup: a rare side reaction. Tuberc Respir Dis. 1991. 38:304–308.7. Calvo E, Fernandez-La Torre F, Brugarolas A. Cervical phrenic nerve block for intractable hiccups in cancer patients. J Natl Cancer Inst. 2002. 94:1175–1176.8. Marechal R, Berghmans T, Sculier P. Successful treatment of intractable hiccup with methylphenidate in a lung cancer patient. Support Care Cancer. 2003. 11:126–128.9. Yang NY, Moon DE, Park CJ, Kwon OK, Park JM, Shim JY, et al. Treatment of intractable hiccup with midazolam and baclofen. Korean J Pain. 1997. 10:246–249.10. Wilcock A, Twycross R. Midazolam for intractable hiccup. J Pain Symptom Manage. 1996. 12:59–61.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Persistent Hiccup after Epidural Steroid Injection: Case reports
- Persistent Hiccups Treatment with Cervical Epidural Block
- A Case of Early Gastric Cancer Associated with Small Cell Lung Cancer
- Persistent Hiccups after Cervical Selective Nerve Root Block
- A Case of Iris Metastasis from Non-small Cell Lung Cancer
