Asymptomatic Right Coronary Artery-to-Pulmonary Artery Fistula Incidentally Detected by Transthoracic Echocardiography
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea. cardiman@medimail.co.kr
- KMID: 1473736
- DOI: http://doi.org/10.4250/jcu.2009.17.3.106
Abstract
- In this case report, we describe a 71-year-old woman with right conal coronary artery-to-pulmonary trunk fistula. She visited the outpatient clinic of the nephrology department for long-term management of renal dysfunction. On transthoracic echocardiography (TTE) conducted as a part of cardiac evaluation, an abnormal Doppler color flow taking a course toward echocardiographic probe was incidentally detected outside the main pulmonary trunk, giving an impression of congenital coronary arteriovenous (AV) fistula. Computed tomography coronary angiography confirmed the presence of congenital coronary AV fistula from a conal branch of the right coronary artery to the main pulmonary trunk in the form of a ground cherry. Although the direction of Doppler color flow is not usual (i.e. toward, not away from, echocardiographic probe) in this case, congenital coronary AV fistula should be in the first priority among potential diagnoses when an abnormal Doppler color flow was found near the main pulmonary trunk on TTE.
MeSH Terms
Figure
-
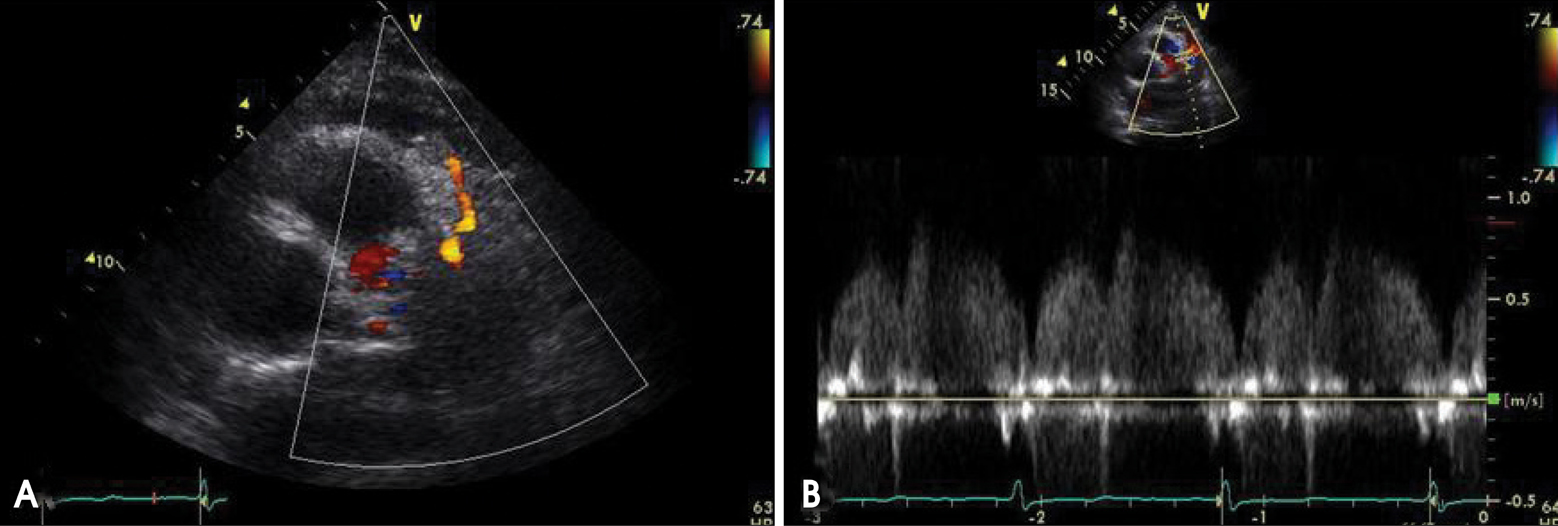
Fig. 1 A: Parasternal short axis view of the patient showing an abnormal Doppler color flow just outside of the main pulmonary trunk. Doppler color flow is directed to the echocardiographic probe (i.e. red color). B: Pulse wave Doppler recording in this abnormal flow reveals predominantly diastolic flow signal, suggesting coronary blood flow.
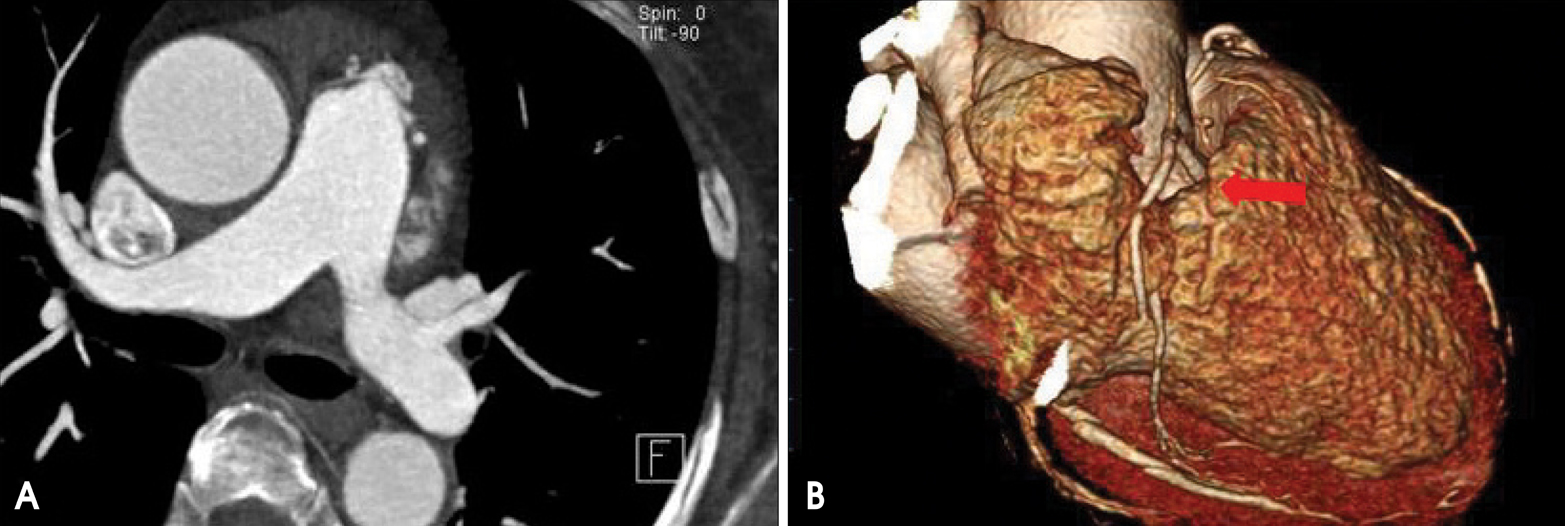
Fig. 2 A: Cross-sectional computed tomography image similar to echocardiographic parasternal short axis view at the aortic valve level. At the left side of the main pulmonary trunk, conglomerated, contrast-enhanced blood vessels without dilatation were observed. B: Three-dimensional image of heart and its coronary artery with contrast-enhanced computed tomographic datasets. Red arrow indicates coronary arteriovenous fistula located close to the main pulmonary trunk in external volume-rendering cardiac image.
Cited by 1 articles
-
Coronary-to-Pulmonary Artery Fistula in Adults: Natural History and Management Strategies
Hokun Kim, Kyongmin Sarah Beck, Yeon Hyeon Choe, Jung Im Jung
Korean J Radiol. 2019;20(11):1491-1497. doi: 10.3348/kjr.2019.0331.
Reference
-
1. Fernandes ED, Kadivar H, Hallman GL, Reul GJ, Ott DA, Cooley DA. Congenital malformations of the coronary arteries: the Texas Heart Institute experience. Ann Thorac Surg. 1992. 54:732–740.
Article2. Lee SJ, Her SH, Jin SW, Lee JM, Yoon HJ, Lee HY, Kim HY, Kim GM, Park CH. A Case of Bilateral Coronary to Pulmonary Artery Fistulas Associated With Severe Aortic Regurgitation. Korean Circ J. 2008. 38:331–334.
Article3. Kim SH, Ko JS, Yoon HJ, Lim SC, Cho SH, Kim HS, Lee JS, Park JC. A Case of Coronary Arteriovenous Fistula Associated with Giant Coronary Artery Aneurysm. J Cardiovasc Ultrasound. 2009. 17:70–72.
Article4. Slater J, Lighty GW Jr., Winer HE, Kahn ML, Kronzon I, Isom OW. Doppler echocardiography and computed tomography in diagnosis of left coronary arteriovenous fistula. J Am Coll Cardiol. 1984. 4:1290–1293.
Article5. Parga JR, Ikari NM, Bustamante LN, Rochitte CE, de Avila LF, Oliveira SA. Case report: MRI evaluation of congenital coronary artery fistulae. Br J Radiol. 2004. 77:508–511.6. Hauser M. Congenital anomalies of the coronary arteries. Heart. 2005. 91:1240–1245.
Article7. Krause W. Uber den Ursprung einer akzessorischen A. coronaria aus der A. pulmonalis. Z Rat Med. 1865. 24:225–229.8. Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006. 107:7–10.
Article9. Vavuranakis M, Bush CA, Boudoulas H. Coronary artery fistulas in adults: incidence, angiographic characteristics, natural history. Cathet Cardiovasc Diagn. 1995. 35:116–120.
Article10. Vitarelli A, De Curtis G, Conde Y, Colantonio M, Di Benedetto G, Pecce P, De Nardo L, Squillaci E. Assessment of congenital coronary artery fistulas by transesophageal color Doppler echocardiography. Am J Med. 2002. 113:127–133.
Article11. Libby P, Bonow RO, Mann DL, Zipes DP. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 2007. 8th ed. W.B. Saunders Company.12. Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978. 58:25–34.
Article13. Lee GB, Gobel FL, Lillehei CW, Neff WS, Eliot RS. Correction of Shunt from Right Conal Coronary Artery to Pulmonary Trunk with Relief of Symptoms. Circulation. 1968. 37:244–248.
Article14. Liberthson RR, Sagar K, Berkoben JP, Weintraub RM, Levine FH. Congenital coronary arteriovenous fistula. Report of 13 patients, review of the literature and delineation of management. Circulation. 1979. 59:849–854.
Article15. Pelliccia A. Congenital coronary artery anomalies in young patients: new perspectives for timely identification. J Am Coll Cardiol. 2001. 37:598–600.16. Balanescu S, Sangiorgi G, Castelvecchio S, Medda M, Inglese L. Coronary artery fistulas: clinical consequences and methods of closure. A literature review. Ital Heart J. 2001. 2:669–676.17. Armsby LR, Keane JF, Sherwood MC, Forbess JM, Perry SB, Lock JE. Management of coronary artery fistulae. Patient selection and results of transcatheter closure. J Am Coll Cardiol. 2002. 39:1026–1032.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Contrast Echo-A Simple Diagnostic Tool for a Coronary Artery Fistula
- A Case of Percutaneous Transcatheter Coil Embolization for Congenital Coronary Arteriovenous Fistula
- Congenital Giant Left Circumflex Artery-to-Left Ventricle Fistula Detected Using Two-Dimensional and Doppler Echocardiography
- Dual Fistulas of Ascending Aorta and Coronary Artery to Pulmonary Artery
- Right Coronary Artery to Left Ventricle Fistula
