J Korean Fract Soc.
2010 Jan;23(1):20-25. 10.12671/jkfs.2010.23.1.20.
Surgical Treatment of AO Type C Distal Femoral Fractures Using Locking Compression Plate (LCP-DF, Synthes(R))
- Affiliations
-
- 1Department of Orthopedic Surgery, Eulji University College of Medicine, Daejeon, Korea. oskkj@eulji.ac.kr
- KMID: 1461568
- DOI: http://doi.org/10.12671/jkfs.2010.23.1.20
Abstract
- PURPOSE
To analyze the surgical results of AO type C distal femoral fractures using locking compression plate.
MATERIALS AND METHODS
From February 2006 to June 2008, 14 patients 15 cases were included. Injury mechanisms, combined injuries, radiologic and clinical results and postoperative complications were analyzed.
RESULTS
The mean age was 59.6 (30~77) years. The mean follow up period was 25 (12~40) months. AO types were 3 of C1, 5 of C2 and 7 of C3. Injury mechanisms were 9 of traffic accident, 5 of slip down and 1 of fall from a height. Four cases were combined with other extremity injuries or fractures. The mean radiologic union was obtained at postoperative 15 (13~20) weeks. The mean Neer's functional score was 74.2 (58~97); 3 of excellent, 5 of satisfactory and 7 of unsatisfactory. Postoperative complications were 2 of infection and 1 of nonunion. There were no mechanical failures or fixation loss with locking compression plate at the final follow up.
CONCLUSION
Internal fixation using locking compression plate for AO type C distal femoral fractures provided excellent fixations. At the final follow up, the clinical results were variable. The affecting factors on the final results seemed to be joint congruencies after anatomical reduction and active rehabilitation.
MeSH Terms
Figure
-

Fig. 1 (A) Initial radiographs show the distal femoral fracture of AO type C3. (B) Initial CT scans show the intra-articular fracture fragments. Sagittal image shows Hoffa fracture fragments. (C) Postoperative radiographs show very congruent articular surface with good alignment. Fracture fragments are reduced and stabilized with locking compression plate and additional Acutrak and cable. (D) Radiographs 16 months after surgery show the healed fracture with callus in good alignment.
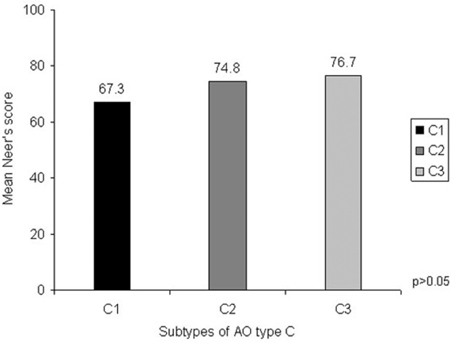
Fig. 2 Mean Neer's functional scores of each subtype of AO type C. It doesn't have statistical significance between subtypes of AO type C and mean Neer's scores.
Reference
-
1. Bolhofner BR, Carmen B, Clifford P. The results of open reduction and internal fixation of distal femur fractures using a biologic (indirect) reduction technique. J Orthop Trauma. 1996. 10:372–377.
Article2. Brown A, D'Arcy JC. Internal fixation for supracondylar fractures of the femur in the elderly patient. J Bone Joint Surg Br. 1971. 53:420–424.
Article3. Choi HR, Song JM, Kwon H, Ko YG, Lee JG, Yoon CH. Operative treatment for AO type C supracondylar fracture of the distal femur. J Korean Soc Fract. 2002. 15:166–172.
Article4. Fracture and dislocation compendium. Orthopaedic Trauma association committee for coding and classification. J Orthop Trauma. 1996. 10:Suppl 1. v–ix. 1–154.5. Haidukewych GJ. Innovations in locking plate technology. J Am Acad Orthop Surg. 2004. 12:205–212.
Article6. Kim SJ, Oh CW, Jeon IH, et al. Minimally invasive plate osteosynthesis for distal femoral fractures. J Korean Soc Fract. 2003. 16:474–481.
Article7. Krettek C, Schandelmaier P, Miclau T, Tscherne H. Minimally invasive percutaneous plate osteosynthesis (MIPPO) using the DCS in proximal and distal femoral fractures. Injury. 1997. 28:Suppl 1. A20–A30.
Article8. Mize RD, Bucholz RW, Grogan DP. Surgical treatment of displaced, comminuted fractures of the distal end of the femur. J Bone Joint Surg Am. 1982. 64:871–879.
Article9. Müller ME, Allgower M, Schneider R, Willenegger H. Manual of internal fixation. Technique recommended by the AO group. 1979. 2nd ed. New York: Springer-Verlag;118–120.10. Neer CS 2nd, Grantham SA, Shelton ML. Supracondylar fracture of the adult femur. A study of one hundred and ten cases. J Bone Joint Surg Am. 1967. 49:591–613.11. Niemeyer P, Südkamp NP. Principles and clinical application of the locking compression plate (LCP). Acta Chir Orthop Traumatol Cech. 2006. 73:221–228.12. Olerud S. Operative treatment of supracondylar--condylar fractures of the femur. Technique and results in fifteen cases. J Bone Joint Surg Am. 1972. 54:1015–1032.13. Russell GV Jr, Smith DG. Minimally invasive treatment of distal femur fractures: report of a technique. J Trauma. 1999. 47:799–801.
Article14. Schatzker J, Tile M. The rationale of operative fracture care. 1996. 3rd ed. New York: Springer-Verlag;415–416.15. Starr AJ, Jones AL, Reinert CM. The "Swashbuckler": a modified anterior approach for fractures of the distal femur. J Orthop Trauma. 1999. 13:138–140.
Article16. Stewart MJ, Sisk TD, Wallace SL. Fractures of the distal third of the femur. A comparison methods of treatment. J Bone Joint Surg Am. 1966. 48:784–807.17. Walling AK, Seradge H, Speigel PG. Injuries to the knee ligaments with fractures of the femur. J Bone Joint Surg Am. 1982. 64:1324–1327.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Medial Plating of Distal Femoral Fracture with Locking Compression Plate-Proximal Lateral Tibia: Cases' Report
- Treatment of Distal Femur Fracture with Minimally Invasive Locking Compression Plate Osteosynthesis
- Analysis of the Result Treated with Locking Compression Plate-Distal Tibia and Zimmer Periarticular Locking Plate in Distal Tibia Fracture
- Comparison of Operative Management in Distal Radius Fractures Using 3.5 mm Versus 2.4 mm Volar Locking Compression Plates
- Comparison of Results of Minimally Invasive Plate Osteosynthesis according to Types of Locking Plate in Distal Femoral Fractures
