A Transthoracic Echocardiographic Follow-Up Study After Catheter Ablation of Atrial Fibrillation: Can We Detect Pulmonary Vein Stenosis by Transthoracic Echocardiography?
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. oys@catholic.ac.kr
- KMID: 1456136
- DOI: http://doi.org/10.4070/kcj.2010.40.9.442
Abstract
- BACKGROUND AND OBJECTIVES
While pulmonary vein isolation (PVI) is an effective curative procedure for patients with atrial fibrillation (AF), pulmonary vein (PV) stenosis is a potential complication which may lead to symptoms that are often unrecognized. The aim of this study was to compare differences between ablation sites in pulmonary venous flow (PVF) measured by transthoracic Doppler echocardiography (TTE) before and after PVI.
SUBJECTS AND METHODS
One hundred five patients (M : F=64 : 41; mean age 56+/-10 years) with paroxysmal AF (n=78) or chronic, persistent AF (n=27) were enrolled. PVI strategies consisted of ostial ablation (n=75; OA group) and antral ablation using an electroanatomic mapping system (n=30; AA group). The ostial diameter was estimated by magnetic resonance imaging (MRI) in patients with PVF > or =110 cm/sec by TTE after PVI.
RESULTS
No patient complained of PV stenosis-related symptoms. Changes in mean peak right PV systolic (-6.7+/-28.1 vs. 10.9+/-25.9 cm/sec, p=0.038) and diastolic (-4.1+/-17.0 vs. 9.9+/-25.9 cm/sec, p=0.021) flow velocities were lower in the AA group than in the OA group. Although the change in mean peak systolic flow velocity of the left PV before and after PVI in the AA group was significantly lower than the change in the OA group (-13.4+/-25.1 vs. 9.2+/-22.3 cm/sec, p=0.016), there was no difference in peak diastolic flow velocity. Two patients in the OA group had high PVF velocities (118 cm/sec and 133 cm/sec) on TTE, and their maximum PV stenoses measured by MRI were 62.5% and 50.0%, respectively.
CONCLUSION
PV stenosis after PVI could be detected by TTE, and PVI by antral ablation using an electroanatomic mapping system might be safer and more useful for the prevention of PV stenosis.
MeSH Terms
Figure
-
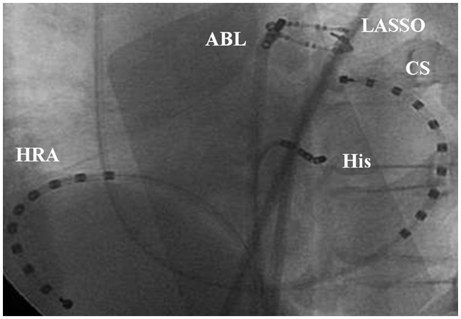
Fig. 1 Fluoroscopic image demonstrating segmental ostial ablation of PV using Lasso guidance. LAO: left anterior oblique view, PV: pulmonary vein; HRA: high right atrium, CS: coronary sinus, ABL: ablation catheter.
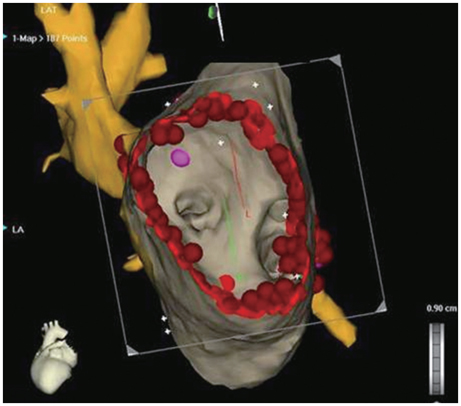
Fig. 2 CARTOMERGE images of LA and PV that have registered a 3-D CT image with the GPS-like CARTO system (endoscopic view). LA: left atrium, PV: pulmonary vein, 3-D CT: 3-dimensional computed tomography, GPS: global positioning system.

Fig. 3 Doppler (A) and MR imaging (B: pre ablation, C: post ablation) of PV in patients with pulmonary vein stenosis that developed after PVI. The white arrow showed significant right superim vein stenosis. MR: magnetic resonance, PV: pulmonary vein, PVI: pulmonary vein isolation.
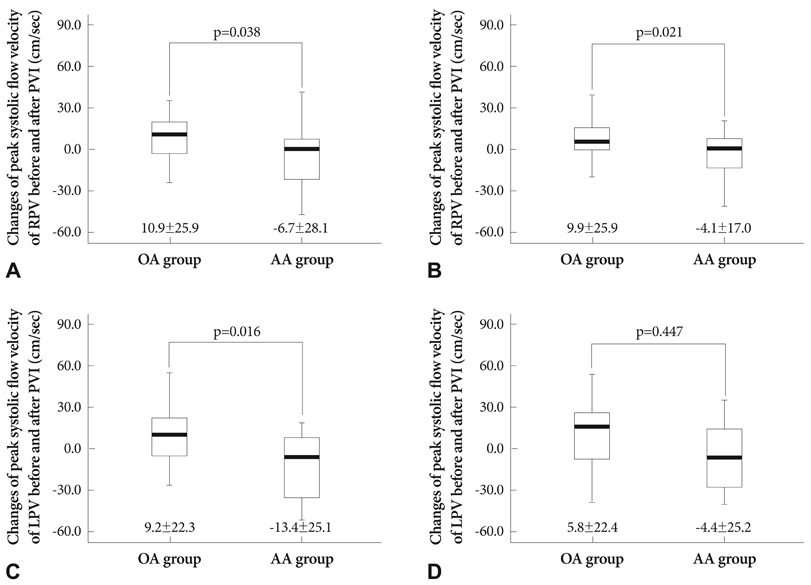
Fig. 4 Changes in peak flow velocity according to ablation sites and use of an electroanatomic (CARTOMERGE) mapping system. This figure shows changes in peak systolic and diastolic flow velocities of RPV (A and B) and LPV (C and D) before and after PVI. RPV: right pulmonary vein, LPV: left pulmonary vein, PVI: pulmonary vein isolation, OA: ostial ablation, AA: antral ablation.
Reference
-
1. Jais P, Haissaguerre M, Shah DC, et al. A focal source of atrial fibrillation treated by discrete radiofrequency ablation. Circulation. 1997. 95:572–576.2. Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998. 339:659–666.3. Kim YH. Rhythm control versus rate control of atrial fibrillation: pharmacologic and non-pharmacologic therapy. Korean Circ J. 2003. 33:553–558.4. Hong GR, Shin DG, Park JS, et al. Effects of pulmonary vein isolation using intraoperative radiofrequency catheter ablation for the treatment of atrial fibrillation associated with mitral valvular heart diseases. Korean Circ J. 2002. 32:596–603.5. Rha SW, Kim YH, Park HN, et al. Initiation and maintenance mechanism of atrial fibrillation assessed by 3-dimensional non-contact mapping system. Korean Circ J. 2004. 34:195–203.6. Robbins IM, Colvin EV, Doyle TP, et al. Pulmonary vein stenosis after catheter ablation of atrial fibrillation. Circulation. 1998. 98:1769–1775.7. Scanavacca MI, Kajita LJ, Vieira M, Sosa EA. Pulmonary vein stenosis complicating catheter ablation of focal atrial fibrillation. J Cardiovasc Electrophysiol. 2000. 11:677–681.8. Yu WC, Hsu TL, Tai CT, et al. Acquired pulmonary vein stenosis after radiofrequency catheter ablation of paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2001. 12:887–892.9. Ernst S, Ouyang F, Goya M, et al. Total pulmonary vein occlusion as a consequence of catheter ablation for atrial fibrillation mimicking primary lung disease. J Cardiovasc Electrophysiol. 2003. 14:366–370.10. Saad EB, Rossillo A, Saad CP, et al. Pulmonary vein stenosis after radiofrequency ablation of atrial fibrillation: functional characterization, evolution and influence of the ablation strategy. Circulation. 2003. 108:3102–3107.11. Haissaguerre M, Jais P, Shah DC, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation. 2000. 101:1409–1417.12. Arentz T, Jander N, von Rosenthal J, et al. Incidence of pulmonary vein stenosis 2 years after radiofrequency catheter ablation of refractory at-rial fibrillation. Eur Heart J. 2003. 24:963–969.13. Pappone C, Rosanio S, Oreto G, et al. Circumferential radiofrequency ablation of pulmonary vein ostia: a new anatomic approach for curing atrial fibrillation. Circulation. 2000. 102:2619–2628.14. Pappone C, Oreto G, Rosanio S, et al. Atrial electroanatomic remodeling after circumferential radiofrequency pulmonary vein ablation: efficacy of an anatomic approach in a large cohort of patients with atrial fibrillation. Circulation. 2001. 104:2539–2544.15. Pappone C, Rosanio S, Augello G, et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: outcomes from a controlled nonrandomized long-term study. J Am Coll Cardiol. 2003. 42:185–197.16. Yu WC, Hsu TL, Tai CT, et al. Acquired pulmonary vein stenosis after radiofrequency catheter ablation of paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2001. 12:887–892.17. Packer DL, Stevens CL, Curley MG, et al. Intracardiac phased-array imaging: methods and initial clinical experience with high resolution, under blood visualization: initial experience with intracardiac phased-array ultrasound. J Am Coll Cardiol. 2002. 39:509–516.18. Saad EB, Rossillo A, Saad CP, et al. Pulmonary vein stenosis after radiofrequency ablation of atrial fibrillation: functional characterization, evolution, and influence of the ablation strategy. Circulation. 2003. 108:3102–3107.19. Jalife J, Berenfeld O, Mansour M. Mother rotors and fibrillatory conduction: a mechanism of atrial fibrillation. Cardiovasc Res. 2002. 54:204–216.20. Jalife J. Rotors and spiral waves in atrial fibrillation. J Cardiovasc Electrophysiol. 2003. 14:776–780.21. Hwang C, Wu TJ, Doshi RN, Peter CT, Chen PS. Vein of marshall cannulation for the analysis of electric activity in patients with focal atrial fibrillation. Circulation. 2000. 101:1503–1505.22. Haissaguerre M, Jais P, Shah DC, et al. Electrophysiological end point for catheter ablation of atrial fibrillation initiated from multiple pulmonary venous foci. Circulation. 2000. 101:1409–1417.23. Lin WS, Tai CT, Hsieh MH, et al. Catheter ablation of paroxysmal atrial fibrillation initiated by non-pulmonary vein ectopy. Circulation. 2003. 107:3176–3183.24. Moe GK. A conceptual model of atrial fibrillation. J Electrocardiol. 1968. 1:145–146.25. Stabile G, Turco P, La Rocca V, Nocerino P, Stabile E, De Simone A. Is pulmonary vein isolation necessary for curing atrial fibrillation? Circulation. 2003. 108:657–660.26. Oral H, Scharf C, Chugh A, et al. Catheter ablation for paroxysmal atrial fibrillation: segmental pulmonary vein ostial ablation versus left atrial ablation. Circulation. 2003. 108:2355–2360.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Controlled Atrial Fibrillation after Pulmonary Vein Stenting
- Role of Echocardiography in Atrial Fibrillation
- Percutaneous Pulmonary Vein Angioplasty for the Pulmonary Vein Stenosis After Catheter Ablation of Atrial Fibrillation
- How to Achieve Complete and Permanent Pulmonary Vein Isolation without Complications
- Echocardiographic Findings of Heart Disease in Children
