Imaging of a Marjolin's Ulcer: A Case Report
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Hospital, Bucheon, Korea. mj4907@schmc.ac.kr
- 2Department of Orthopedics, Seoul SKY Hospital, Korea.
- 3Department of Pathology, Soonchunhyang University Hospital, Bucheon, Korea.
- KMID: 1443510
- DOI: http://doi.org/10.3348/jksr.2011.64.6.593
Abstract
- A Marjolin's ulcer refers to malignancies that developed in chronic venous ulcers, scars, or sinuses. We report three-dimensional computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET)-CT findings in a patient who developed skin cancer from a chronic leg ulcer. Although rare, on MR, a Marjolin's ulcer should be considered when a well-enhanced soft-tissue mass with a broad based skin ulcer shows a mass effect and invasion of the adjacent bone. CT angiography and PET-CT complement MRI for evaluating the nature of Marjolin's ulcers and may provide essential anatomical information, enabling the physician to design the optimal surgical approach or determining cancer staging.
MeSH Terms
Figure
-

Fig. 1 Anteroposterior radiograph of the left lower leg shows cortical thickening of the fibular diaphysis (arrowheads) beneath the skin ulcer (arrow). Note the cortical hypertrophy on the opposite side of the skin ulcer.
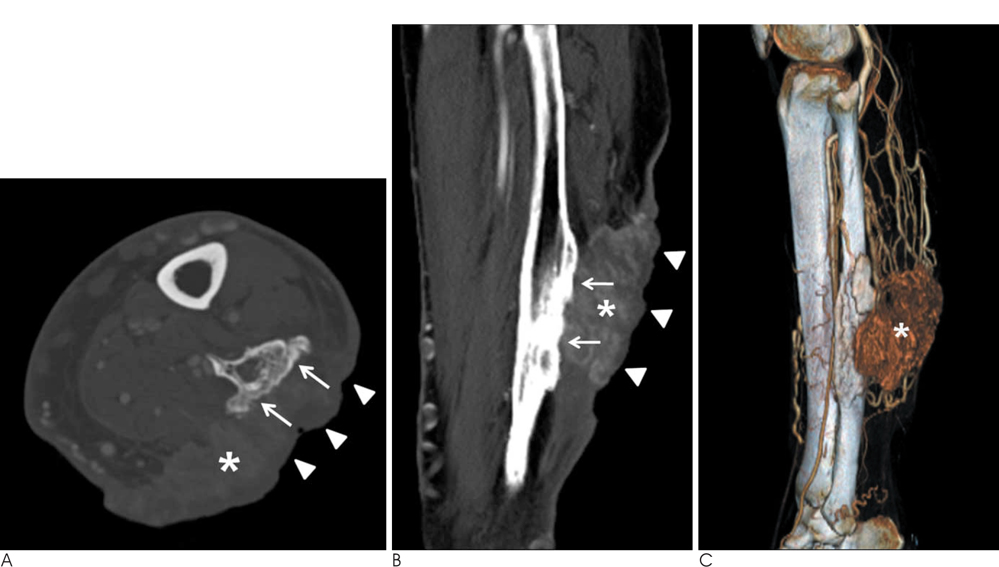
Fig. 2 Computed tomography. A. Axial CT with bone setting reveals cortical hypertrophy of the left lateral fibula (arrows) extending anteroposteriorly parallel to the skin ulcer (arrowheads). A soft tissue mass (asterisk) is also seen between the skin ulcer and fibula. B. Sagittal reformatted contrast-enhanced CT shows a thickened cortex (arrows), which is extrinsically eroded by a soft-tissue mass (asterisk) with a broad base on the skin ulcer (arrowheads). C. CT angiography with color-coded volume-rendering demonstrates a well-enhanced soft-tissue mass (asterisk) surrounded by numerous supplying arteries.
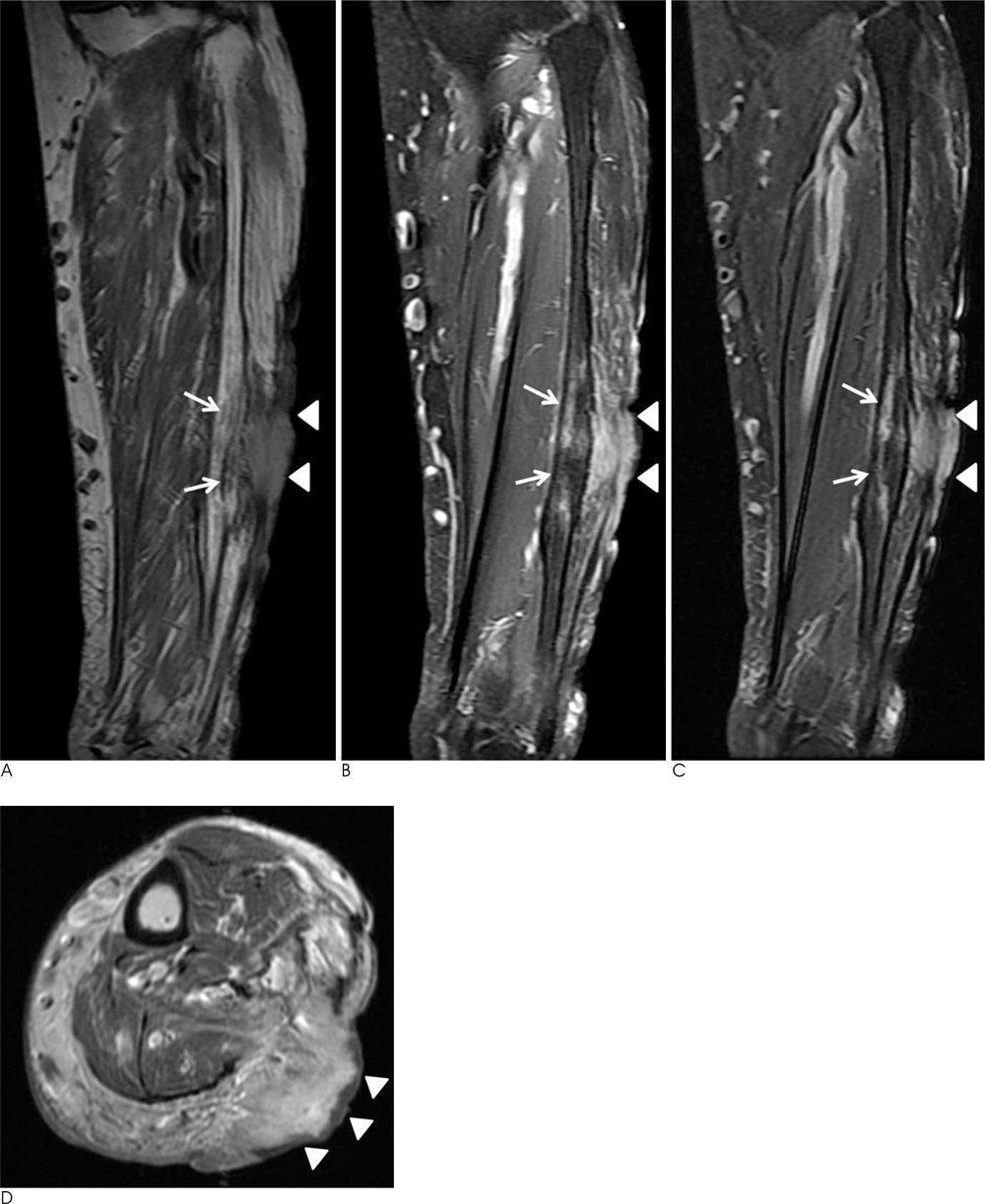
Fig. 3 Magnetic resonance imaging. A-C. The soft tissue mass (arrowheads) shows slightly greater signal intensity than muscle on (A) coronal T1weighted images [repetition time (TR) 1466, echo time (TE) 15], (B) high signal intensity on fat-saturated T2-weighted images (TR 3550, TE 65), and (C) strong enhancement on contrast enhanced fat saturated T1-weighted images (TR 833,TE 13). Note the cortical involvement of the soft tissue mass and abnormal signal intensity lesions in the bone marrow (arrows). D. The axial contrast-enhanced T1-weighted image (TR 900, TE 11) shows a highly homogenous enhanced mass bulging out from the skin scar.

Fig. 4 PET/CT. Transverse PET/CT shows intense FDG uptake by the soft tissue mass (arrowheads), which is seen as a highly enhanced mass on CT and MR images. There was no abnormal FDG uptake in the bone marrow where abnormal signal intensity was seen on MRI.
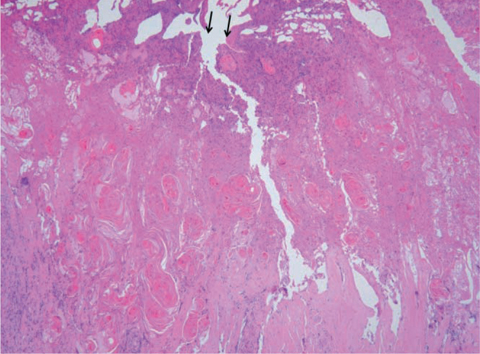
Fig. 5 Microscopically, nests of atypical squamous cells with keratinization spread from the ulcerated epidermis (arrows) into the deep dermis (hematoxylin and eosin staining; original magnification, × 40).
Reference
-
1. Smith J, Mello LF, Nogueira Neto NC, Meohas W, Pinto LW, Campos VA, et al. Malignancy in chronic ulcers and scars of the leg (Marjolin's ulcer): a study of 21 patients. Skeletal Radiol. 2001; 30:331–337.2. Chiang KH, Chou AS, Hsu YH, Lee SK, Lee CC, Yen PS, et al. Marjolin's ulcer: MR appearance. AJR Am J Roentgenol. 2006; 186:819–820.3. Rieger UM, Kalbermatten DF, Wettstein R, Heider I, Haug M, Pierer G. Marjolin's ulcer revisited--basal cell carcinoma arising from grenade fragments? Case report and review of the literature. J Plast Reconstr Aesthet Surg. 2008; 61:65–67.4. Kolawole TM, Bohrer SP. Ulcer osteoma-bone response to tropical ulcer. Am J Roentgenol Radium Ther Nucl Med. 1970; 109:611–618.5. Karasick D, Schweitzer ME, Deely DM. Ulcer osteoma and periosteal reactions to chronic leg ulcers. AJR Am J Roentgenol. 1997; 168:155–157.6. Pretorius ES, Fishman EK. Volume-rendered three-dimensional spiral CT: Musculoskeletal applications. Radiographics. 1999; 19:1143–1160.7. Shin DS, Shon OJ, Han DS, Choi JH, Chun KA, Cho IH. The clinical efficacy of (18)F-FDG PET/CT in benign and malignant musculoskeletal tumors. Ann Nucl Med. 2008; 22:603–609.8. Feldman F, van Heertum R, Manos C. 18-FDG PET scanning of benign and malignant musculoskeletal lesions. Skeletal Radiol. 2003; 32:201–208.9. Aoki J, Watanabe H, Shinozaki T, Takagishi K, Tokunaga M, Koyama Y, et al. FDG-PET for preoperative differential diagnosis between benign and malignant soft tissue masses. Skeletal Radiol. 2003; 32:133–138.10. Fleming MD, Hunt JL, Purdue GF, Sandstad J. Marjolin's ulcer: a review and reevaluation of a difficult problem. J Burn Care Rehabil. 1990; 11:460–469.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Marjolin's Ulcer Secondary to Tuberculous Tenosynovitis of the Wrist: A Case Report
- A clinical analysis of the marjolin's ulcer
- Marjolin's Ulcer Presenting with In-Transit Metastases: A Case Report and Literature Review
- Squamous Cell Carcinoma Occurring at the Site of an Arteriovenous Fistula Ulcer: A Case Report
- Outcomes of Treatment for Squamous Cell Carcinoma Originating as a Marjolin's Ulcer
