A Pictorial Review on Extraosseous Manifestations of Multiple Myelomas
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. kyungs.lee@samsung.com
- KMID: 1443506
- DOI: http://doi.org/10.3348/jksr.2011.64.6.567
Abstract
- Extraosseous involvement of multiple myelomas can be seen clinically or radiologically in approximately 10-20% of patients at the time of initial diagnosis and may develop in an additional 15% of patients over the course of the disease. The condition can arise in any tissue of the body and its presence has been associated with more aggressive disease, a guarded prognosis, or high-dose chemotherapy. Imaging findings of extraosseous multiple myelomas are diverse. They usually show high enhancement on contrast-medium enhanced CT scans, exhibit iso-signal intensity on both T1- and T2-weighted images, and variable 18F-fluorine deoxyglucose (FDG) uptake at PET. The disease may simulate an infectious condition since it may be concurrent with underlying multiple myelomas per se or it may occur during myeloma treatment including stem cell transplantation.
MeSH Terms
Figure
-
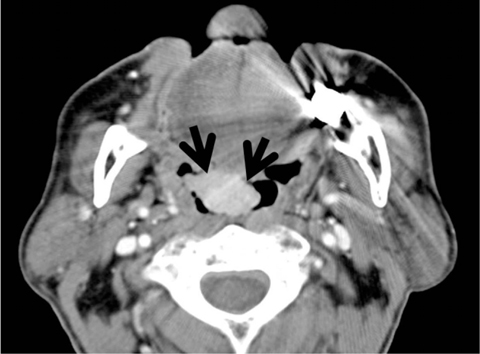
Fig. 1 Biopsy-proven plasmacytoma in the oropharynx of a 76-year-old man with IgG multiple myeloma. A contrast enhanced CT scan at the level of the tongue base shows a homogenous, well-enhancing, soft-tissue mass (arrows) in the anterior wall of oropharynx.
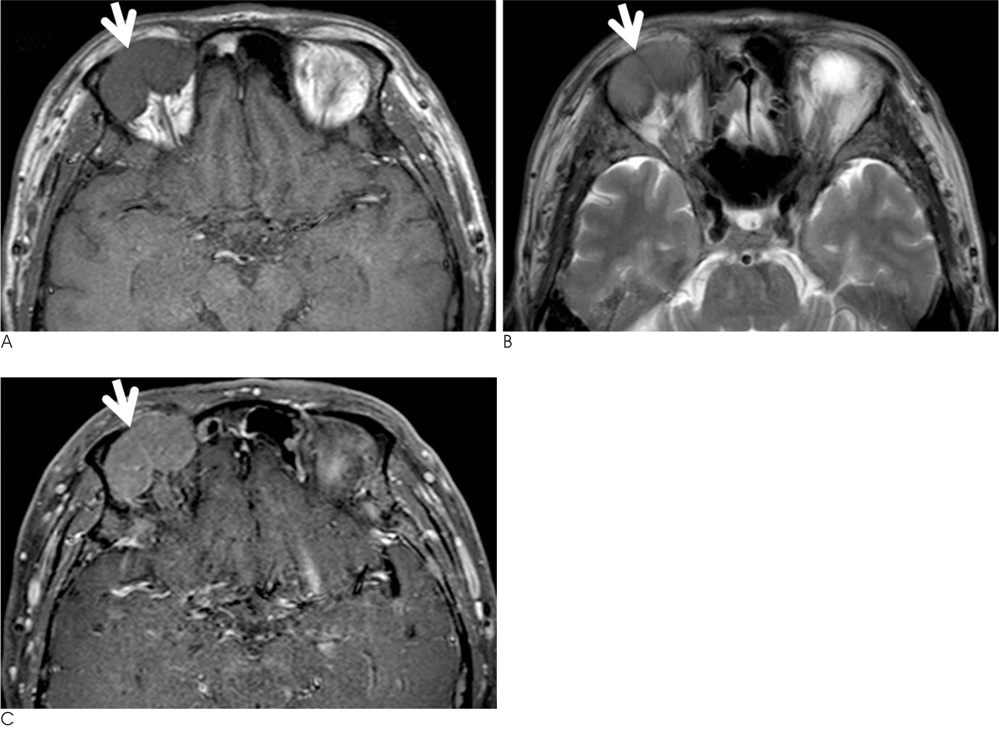
Fig. 2 An ocular myeloma in a 60-year-old man with extensive systemic manifestation of IgM multiple myeloma. A, B. T1-weighted (A) and T2-weighted (B) MR images show an iso-signal intensity lesion (arrows) in the right eye orbit. C. A contrast-enhanced T1-weighted MR image demonstrates homogenous enhancement (arrow) of the lesion.
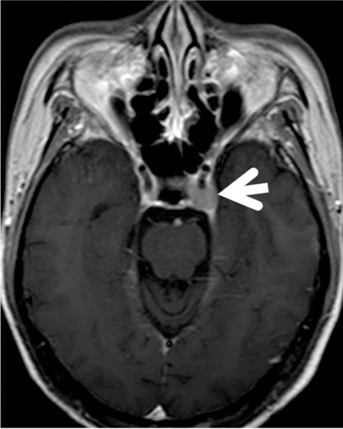
Fig. 3 Cavernous sinus κlight-chain myeloma in a 58-year-old woman. A contrast enhanced T1-weighted MR image shows a newly developed soft-tissue nodule (arrow) in the left cavernous sinus. The lesion was absent on MR images obtained one year ago. CSF analysis revealed atypical plasmacytoid cells.
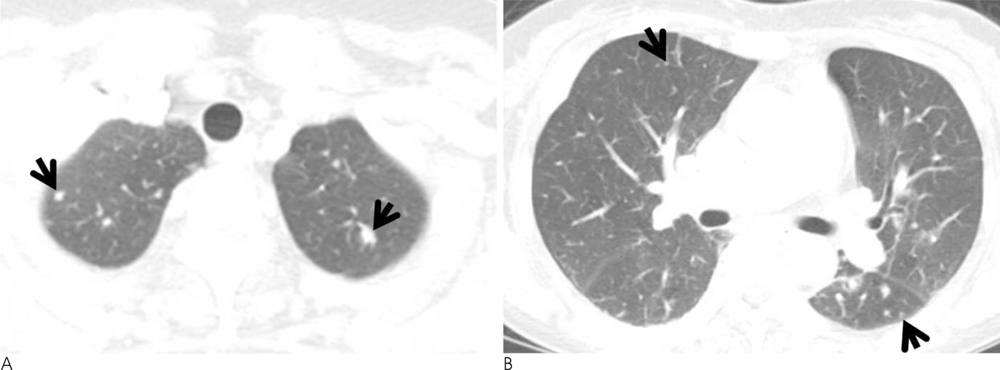
Fig. 4 Pulmonary κlight-chain myelomas in a 58-year-old woman. A, B. Conventional CT images (5.0-mm-section thickness) obtained at the levels of thoracic inlet (A) and bronchus intermedius (B), respectively, show multiple variable sized lung nodules (arrows) scattered in both lungs. Lung lesions were considered to infer lung involvement of multiple myeloma due to the absence of signs of infection and regression after chemotherapy (not shown here). Small amounts of bilateral pleural effusions were also seen. Plasma cells were identified in a pleural fluid analysis.

Fig. 5 Pleural IgM myeloma in a 60-year-old man. Enhanced CT scan (2.5-mm-section thickness) obtained at the atrial level shows bilateral pleural effusions. Also note the multifocal areas of pleural thickening and mass-like lesions (arrows).

Fig. 6 Biopsy-proven mediastinal λlight-chain myeloma in a 45-year-old man. A. Chest radiograph shows bilateral mediastinal widening (arrows). B. A contrast-enhanced CT scan (2.5-mm-section thickness) obtained at the level of the main bronchi demonstrates a large bilateral anterior mediastinal mass that shows mild enhancement. Small amounts of bilateral pleural effusions, small in amount are also associated. A surgical biopsy specimen revealed a myelomatous lesion. (Min JH, et al. J Korean Soc Radiol 2010;62:365-368, with permission)
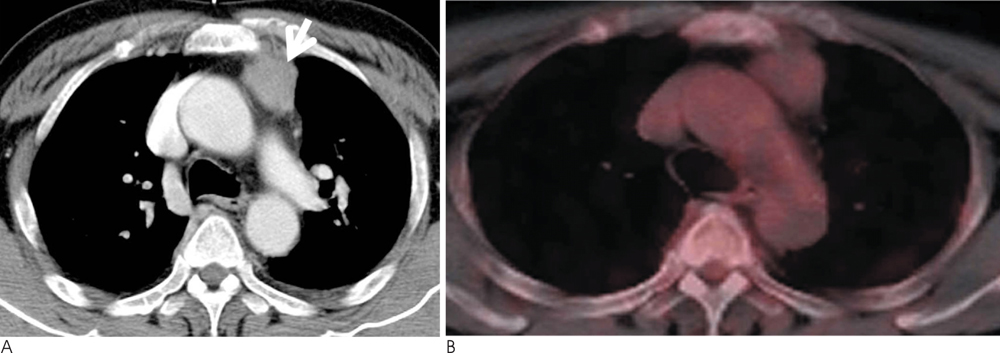
Fig. 7 Biopsy-proven mediastinal IgD myeloma in a 60-year-old man. A. A contrast-enhanced CT scan (5.0-mm-section thickness) obtained at the level of the azygos arch shows an enhancing left anterior mediastinal mass (arrow). B. PET scan obtained at a similar level to a demonstrates little FDG uptake within the lesion. After chemotherapy, the left anterior mediastinal mass disappeared (not shown here).

Fig. 8 Biopsy-proven hepatic λlight-chain myelomas in a 49-year-old woman who is a hepatitis-B virus carrier. A. Ultrasonography of the liver shows multiple hypoechoic nodules (arrows) in both lobes of the liver. B, C. Enhanced liver CT scans obtained at the levels of the liver dome (B) and hepatic veins (C), respectively, and in the portal phase, show enhancing small hepatic nodules (arrows) in both lobes of the liver. D. T2-weighted MR image shows multiple hyperintense nodular lesions (arrows) in the liver. E. Dynamic MR images obtained after the injection of gadoxetic acid show multiple nodules in the liver. The nodules show enhancement at the arterial phase (A) and washout in both the equilibrium (E) and hepatobiliary (H) phases.

Fig. 9 Biopsy-proven hepatic IgD myelomas in 69-year-old man. A. An enhanced whole-body MR image shows iso- to slightly high-signal intensity lesions (arrows, osseous involvement of myeloma) in the right proximal and distal tibia. Also noted is a round lesion (arrowhead) in the liver with slightly lower-signal intensity than normal liver. The hepatic lesion showed early arterial enhancement and delayed washout on dynamic MR images as in Figure 8 (not shown here). B. A PET scan does not show any evidence of FDG uptake either in bone lesions in the right tibia or in the liver lesion.

Fig. 10 Renal involvement of λlight-chain myeloma in a 49-year-old woman. Newly developed multifocal low-attenuation lesions (arrows) are observed in both kidneys on delayed-phase CT images. Patients had such renal lesions on regular follow-up CT studies after the complete remission of multiple myeloma.
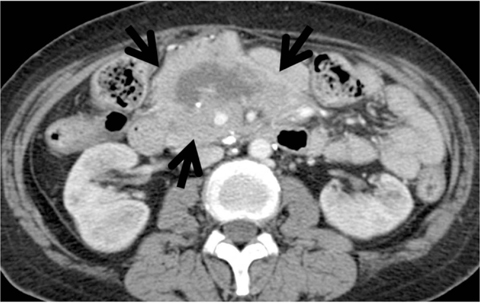
Fig. 11 Mesenteric IgG and λlight-chain myeloma in a 51-year-old woman. Contrast enhanced CT scan (5.0-mm-section thickness) shows a large mass lesion (arrows) within the mesenteries. The lesion harbors a central necrotic portion, and entraps the superior mesenteric vessels. Plasmacytoma was histopathologically confirmed.

Fig. 12 Retroperitoneal IgG and κlight-chain myeloma in a 68-year-old woman. A contrast-enhanced CT scan (5.0-mm-section thickness) shows a highly enhancing infiltrative mass (arrows) in the presacral and right parapelvic areas. A double-J catheter (arrowhead) was inserted into the right ureter, owing to its invasion by the mass.
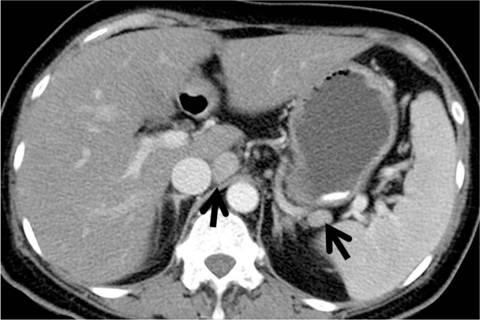
Fig. 13 Lymph node involvement of λlight-chain myeloma in a 49-year-old woman. A contrast-enhanced CT scan (5.0-mm-section thickness) obtained at the level of porta hepatis shows enlarged lymph nodes (arrows) around the caudate lobe of the liver and splenic artery, respectively. The lesions were absent on CT scans (not shown here) taken two years ago.

Fig. 14 Psoas muscle κlight-chain myeloma in a 48-year-old woman. A contrast enhanced CT scan (5.0-mm-section thickness obtained at the level of pelvic inlet shows a heterogeneously enhancing mass lesion (arrows) in the right psoas muscle. Also note a smaller enhancing lesion (arrowhead) in the right iliacus muscle area.
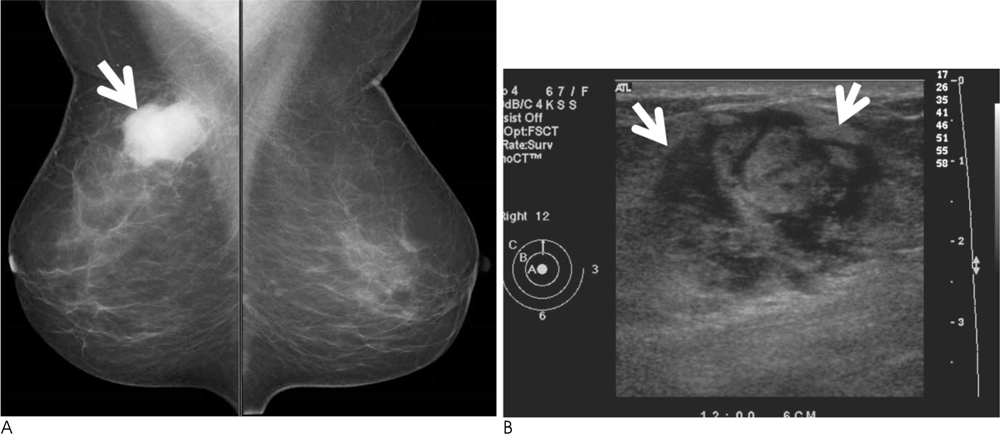
Fig. 15 Breast IgG and κlight-chain myeloma in a 65-year-old woman. A. Mediolateral oblique view of mammography shows a well-circumscribed hyperdense mass (arrow) in the upper central portion of the right breast. B. Ultrasonography of right breast shows a heterogeneous low-echoic mass (arrows) in the corresponding mammographic area.
Cited by 1 articles
-
Central Nervous System Involvement in a Patient with Multiple Myeloma Manifesting as an Intraventricular Mass with Leptomeningeal Spread
Jung Eun Lee, Eun Ja Lee, Hee Jin Huh, Jae-Woo Chung, Eun Kyoung Lee, Hyun Jung Lee
J Korean Soc Radiol. 2018;79(1):50-55. doi: 10.3348/jksr.2018.79.1.50.
Reference
-
1. Varettoni M, Corso A, Pica G, Mangiacavalli S, Pascutto C, Lazzarino M. Incidence, presenting features and outcome of extramedullary disease in multiple myeloma: a longitudinal study on 1003 consecutive patients. Ann Oncol. 2010; 21:325–330.2. Moulopoulos LA, Granfield CA, Dimopoulos MA, Kim EE, Alexanian R, Libshitz HI. Extraosseous multiple myeloma: imaging features. AJR Am J Roentgenol. 1993; 161:1083–1087.3. Patlas M, Hadas-Halpern I, Libson E. Imaging findings of extraosseous multiple myeloma. Cancer Imaging. 2002; 2:120–122.4. Hall MN, Jagannathan JP, Ramaiya NH, Shinagare AB, Van den Abbeele AD. Imaging of extraosseous myeloma: CT, PET/CT, and MRI features. AJR Am J Roentgenol. 2010; 195:1057–1065.5. Damaj G, Mohty M, Vey N, Dincan E, Bouabdallah R, Faucher C, et al. Features of extramedullary and extraosseous multiple myeloma: a report of 19 patients from a single center. Eur J Haematol. 2004; 73:402–406.6. Patriarca F, Zaja F, Silvestri F, Sperotto A, Scalise A, Gigli G, et al. Meningeal and cerebral involvement in multiple myeloma patients. Ann Hematol. 2001; 80:758–762.7. Masood A, Hudhud KH, Hegazi A, Syed G. Mediastinal plasmacytoma with multiple myeloma presenting as a diagnostic dilemma. Cases J. 2008; 1:116.8. Patlas M, Khalili K, Dill-Macky MJ, Wilson SR. Spectrum of imaging findings in abdominal extraosseous myeloma. AJR Am J Roentgenol. 2004; 183:929–932.9. Goh J, Otridge B, Brady H, Breatnach E, Dervan P, MacMathuna P. Aggressive multiple myeloma presenting as mesenteric panniculitis. Am J Gastroenterol. 2001; 96:238–241.10. Oshima K, Kanda Y, Nannya Y, Kaneko M, Hamaki T, Suguro M, et al. Clinical and pathologic findings in 52 consecutively autopsied cases with multiple myeloma. Am J Hematol. 2001; 67:1–5.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Systemic Manifestations of Immunoglobulin G4-Related Disease: A Pictorial Essay
- Extraosseous Tuberculosis of the Extremities
- A Case of Extradural Spinal Tuberculoma
- Extraosseous Ewing sarcoma of the pancreas: a case report
- Neurological Complications Following Liver Transplant: A Pictorial Review of Radiological and Clinical Findings
