Relationship of Pelvic Bone Fracture Pattern and Bleeding Foci on Angiography
- Affiliations
-
- 1Department of Radiology, Gachon University School of Medicine, Gil Hospital, Incheon, Korea. ho7ok7@gilhospital.com
- KMID: 1439541
- DOI: http://doi.org/10.3348/jksr.2012.67.4.277
Abstract
- PURPOSE
The purpose of this study is to evaluate the relationship between the patterns of pelvic bone fracture and location of hemorrhage on angiography.
MATERIALS AND METHODS
We retrospectively reviewed 56 patients with pelvic bone fracture and active bleeding. Fractures were classified according to Tile classification. Locations of bleedings were divided into four groups; main trunk/anterior/posterior divisions of internal iliac artery, and other locations. The relationship between the fracture pattern and bleedings were analyzed statistically.
RESULTS
Forty-one bleedings were in 22 patients with type A fracture. Twenty (49%) were at the anterior division, 12 (29%) were at the posterior division, and 9 (22%) were found in other location. Thirty-three bleedings were in 23 patients with type B fracture. Fifteen (45%) were at the posterior division, 10 (30%) were at the anterior division, 3 (9%) were at the main trunk of the internal iliac artery, and 5 (16%) were at other location. Eighteen bleedings were in 11 patients with type C fracture. Thirteen (72%) were at the posterior division, 4 (22%) were at the anterior division, and 1 (6%) was at main trunk of internal iliac artery. Anterior divisional bleedings were more common in type A, posterior divisional bleedings were more common in type B and C fractures (p = 0.014).
CONCLUSION
The distribution of bleeding is significantly related to the fracture patterns. Fracture pattern may help in predicting the location of bleeding foci on embolization.
Figure
-

Fig. 1 A 35-year-old male who has a compression injury on the lower abdomen. A. Conventional pelvic AP view shows minimally displaced pubic bone fracture (arrows) suggestive of type A fracture. B. Angiography shows contrast extravasation in the right obturator artery, a branch of the internal iliac artery anterior division (arrowhead). Note.-AP = anteroposterior
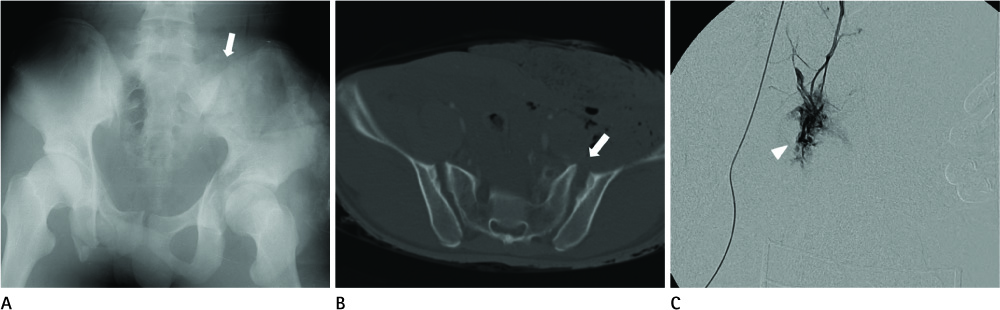
Fig. 2 An 18-year-old male who had an motorcycle accident. A, B. Conventional pelvic AP view and abdominopelvic CT shows fracture of the right pubic ramus and disrupted anterior margin of the left sacroiliac joint (arrows), suggestive of type B fracture. C. Angiography shows active bleeding at the left main internal iliac artery (arrowhead). Note.-AP = anteroposterior
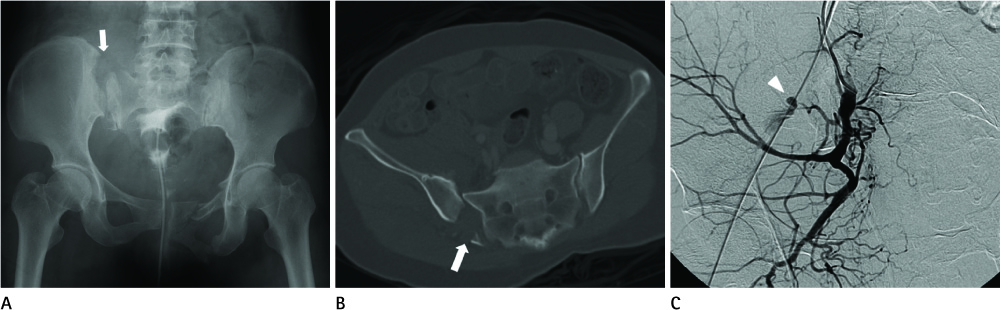
Fig. 3 A 50-year-old female who was involved in a pedestrian-traffic accident. A, B. Conventional pelvic AP view and abdominopelvic CT shows complete disruption of the right sacroiliac joint with vertical and rotational instability, suggestive of type C fracture (arrows). C. Angiography shows active bleeding at the right superior gluteal artery, a branch of the internal iliac artery posterior division (arrowhead). Note.-AP = anteroposterior
Reference
-
1. Yoon W, Kim JK, Jeong YY, Seo JJ, Park JG, Kang HK. Pelvic arterial hemorrhage in patients with pelvic fractures: detection with contrast-enhanced CT. Radiographics. 2004; 24:1591–1605. discussion 1605-16062. Fu CY, Wu SC, Chen RJ, Wang YC, Chung PK, Yeh CC, et al. Evaluation of pelvic fracture stability and the need for angioembolization: pelvic instabilities on plain film have an increased probability of requiring angioembolization. Am J Emerg Med. 2009; 27:792–796.3. Salim A, Teixeira PG, DuBose J, Ottochian M, Inaba K, Margulies DR, et al. Predictors of positive angiography in pelvic fractures: a prospective study. J Am Coll Surg. 2008; 207:656–662.4. Ben-Menachem Y, Coldwell DM, Young JW, Burgess AR. Hemorrhage associated with pelvic fractures: causes, diagnosis, and emergent management. AJR Am J Roentgenol. 1991; 157:1005–1014.5. Anderson SW, Soto JA, Lucey BC, Burke PA, Hirsch EF, Rhea JT. Blunt trauma: feasibility and clinical utility of pelvic CT angiography performed with 64-detector row CT. Radiology. 2008; 246:410–419.6. Cerva DS Jr, Mirvis SE, Shanmuganathan K, Kelly IM, Pais SO. Detection of bleeding in patients with major pelvic fractures: value of contrast-enhanced CT. AJR Am J Roentgenol. 1996; 166:131–135.7. Pinto A, Niola R, Tortora G, Ponticiello G, Russo G, Di Nuzzo L, et al. Role of multidetector-row CT in assessing the source of arterial haemorrhage in patients with pelvic vascular trauma. Comparison with angiography. Radiol Med. 2010; 115:648–667.8. Shanmuganathan K, Mirvis SE, Sover ER. Value of contrast-enhanced CT in detecting active hemorrhage in patients with blunt abdominal or pelvic trauma. AJR Am J Roentgenol. 1993; 161:65–69.9. Mouzopoulos G, Tzurbakis M, Mouzopoulos D, Ierodiakonou V, Tsembeli A, Georgilas I. Massive haemorrhage due to minimally displaced pubic ramus fracture. Eur J Emerg Med. 2009; 16:271–272.10. Lopez PP. Unstable pelvic fractures: the use of angiography in controlling arterial hemorrhage. J Trauma. 2007; 62:6 Suppl. S30–S31.11. Fang JF, Shih LY, Wong YC, Lin BC, Hsu YP. Repeat transcatheter arterial embolization for the management of pelvic arterial hemorrhage. J Trauma. 2009; 66:429–435.12. Stambaugh LE 3rd, Blackmore CC. Pelvic ring disruptions in emergency radiology. Eur J Radiol. 2003; 48:71–87.13. Magnussen RA, Tressler MA, Obremskey WT, Kregor PJ. Predicting blood loss in isolated pelvic and acetabular high-energy trauma. J Orthop Trauma. 2007; 21:603–607.14. Frevert S, Dahl B, Lönn L. Update on the roles of angiography and embolisation in pelvic fracture. Injury. 2008; 39:1290–1294.15. Zhang Q, Chen W, Smith WR, Pan J, Liu H, Zhang Y. Superior gluteal artery injury presenting as delayed onset shock. Arch Orthop Trauma Surg. 2010; 130:251–256.16. Metz CM, Hak DJ, Goulet JA, Williams D. Pelvic fracture patterns and their corresponding angiographic sources of hemorrhage. Orthop Clin North Am. 2004; 35:431–437. v17. O'Neill PA, Riina J, Sclafani S, Tornetta P 3rd. Angiographic findings in pelvic fractures. Clin Orthop Relat Res. 1996; 60–67.18. Hamill J, Holden A, Paice R, Civil I. Pelvic fracture pattern predicts pelvic arterial haemorrhage. Aust N Z J Surg. 2000; 70:338–343.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of Ongoing Bleeding after a Damage Control Laparotomy for a Pelvic Bone Fracture: Arterial Embolization: A Case Report
- Retroperitoneal Gauze Packing with Vacuum-Associated Closure for Pelvic Fracture with Hemodynamic Instability
- Comparisons of Fracture Types and Pelvic Angiographic Findings in Hemodynamically Unstable Pelvic Bone Fracture
- Transcatheter Arterial Embolizations of Arterial Bleeding in Patients with Pelvic Bone Fracture
- Blush on Computed Tomography and Transcatheter Arterial Embolization in Pelvic Fracture
