A Case of Macrophagic Myofasciitis Initially Thought to Be a Metastatic Infection
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Seoul National University, Seoul, Korea. elee@snu.ac.kr
- 2Department of Pathology, College of Medicine, Seoul National University, Seoul, Korea.
- KMID: 1438538
- DOI: http://doi.org/10.4078/jrd.2012.19.5.285
Abstract
- Macrophagic myofasciitis (MMF) is a rare disease, often associated with the pathological persistence of aluminum hydroxide used in some vaccines, and is characterized by macrophage infiltration of the muscle. We report a case of MMF, initially thought to be a metastatic infection. A 38-year-old woman presented with fever, as well as pain and weakness in both thighs. On physical examination both thighs were swollen and lower-extremity motor-power was decreased to grade III. Laboratory tests showed leukocytosis and elevation of acute phase reactants, but all muscle enzymes except lactate dehydrogenase (LDH) were within normal range. Initially metastatic infection was suspected but she was diagnosed with MMF by muscle biopsy showing heavy CD68 positive macrophage infiltration. Her myalgia and muscle weakness improved after systemic steroid treatment. This case suggests that MMF might be considered for a patient with unexplained inflammatory myopathy with or without a history of vaccination.
Keyword
MeSH Terms
-
Acute-Phase Proteins
Adult
Aluminum Hydroxide
Biopsy
Fasciitis
Female
Fever
Humans
Hydroxides
L-Lactate Dehydrogenase
Leukocytosis
Macrophages
Muscle Weakness
Muscles
Myositis
Physical Examination
Rare Diseases
Reference Values
Thigh
Vaccination
Vaccines
Acute-Phase Proteins
Aluminum Hydroxide
Fasciitis
Hydroxides
L-Lactate Dehydrogenase
Myositis
Vaccines
Figure
-
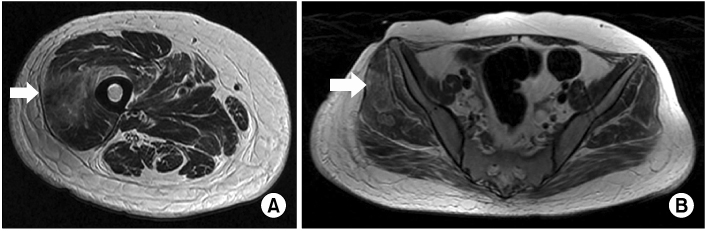
Figure 1 (A) MRI Rt Thigh AXL FSE T2 and (B) MRI Hip AXL FSE T2 gadolinium enhanced show multifocal peripheral rim enhancing lesions (arrow) with perilesional edema involving (A) the right vastus lateralis, (B) bilateral gluteus muscles and intermedius muscles.
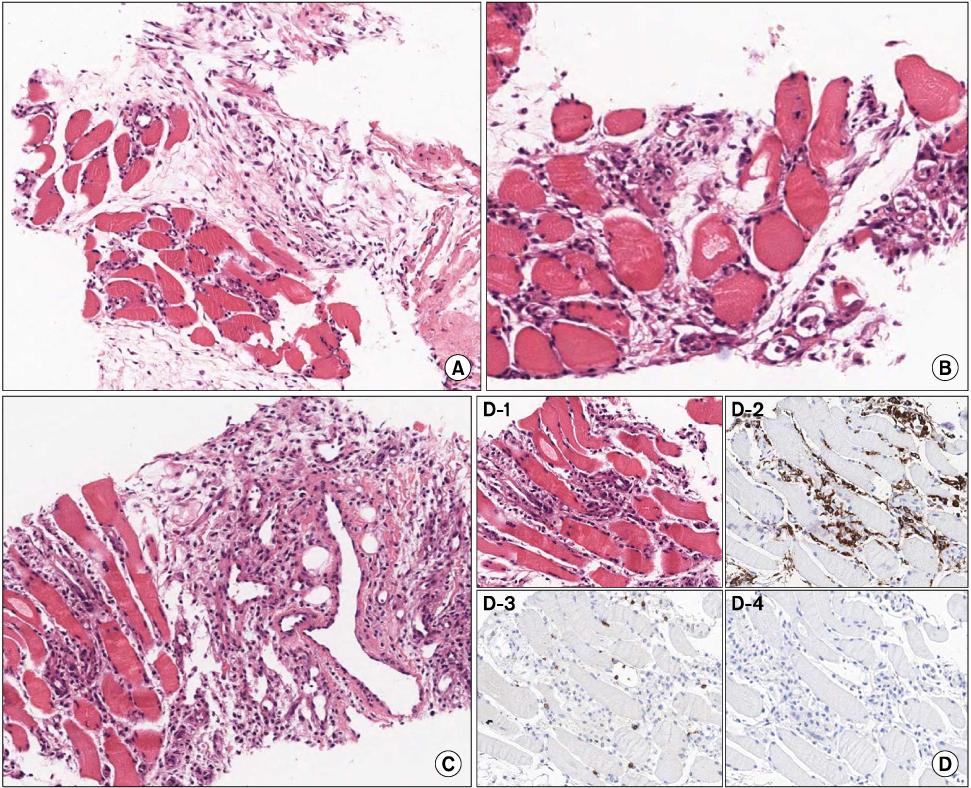
Figure 2 Gun biopsy at right gluteus medius specimen shows severe atrophy, degeneration and regeneration of muscle fibers. Endomyseal fibrosis and fat ingrowth is evident (A, ×200, H&E). Macrophage infiltratioin of the endomysium, degenerating myofibers (B, ×200, H&E) and perivascular areas, but there are no vasculitis (C, ×200, H&E). Macrophage infiltration in myofibers is shown in H&E stain (D-1, ×400). Macrophages are positive for CD68 immunohistochemistry (D-2). There are a few CD3 positive T lymphocytes (D-3) but no B lymphocytes in CD20 stain (D-4).
Reference
-
1. Gherardi RK, Coquet M, Chérin P, Authier FJ, Laforêt P, Bélec L, et al. Macrophagic myofasciitis: an emerging entity. Groupe dEtudes et Recherche sur les Maladies Musculaires Acquises et Dysimmunitaires (GERMMAD) de l'Association Française contre les Myopathies (AFM). Lancet. 1998. 352:347–352.2. Authier FJ, Cherin P, Creange A, Bonnotte B, Ferrer X, Abdelmoumni A, et al. Central nervous system disease in patients with macrophagic myofasciitis. Brain. 2001. 124:974–983.3. Cherin P, Gherardi RK. Macrophagic myofasciitis. Curr Rheumatol Rep. 2000. 2:196–200.4. Gherardi RK, Coquet M, Cherin P, Belec L, Moretto P, Dreyfus PA, et al. Macrophagic myofasciitis lesions assess long-term persistence of vaccine-derived aluminium hydroxide in muscle. Brain. 2001. 124:1821–1831.5. Ryan AM, Bermingham N, Harrington HJ, Keohane C. Atypical presentation of macrophagic myofasciitis 10 years post vaccination. Neuromuscul Disord. 2006. 16:867–869.6. Park JH, Na KS, Park JH, Park YW, Paik SS, Yoo DH. Macrophagic myofasciitis unrelated to vaccination. Scand J Rheumatol. 2005. 34:65–67.7. Rimaniol AC, Gras G, Verdier F, Capel F, Grigoriev VB, Porcheray F, et al. Aluminum hydroxide adjuvant induces macrophage differentiation towards a specialized antigen-presenting cell type. Vaccine. 2004. 22:3127–3135.8. Guis S, Pellissier JF, Nicoli F, Reviron D, Mattei JP, Gherardi RK, et al. HLA-DRB1*01 and macrophagic myofasciitis. Arthritis Rheum. 2002. 46:2535–2537.9. Guis S, Mattéi JP, Lioté F. Drug-induced and toxic myopathies. Best Pract Res Clin Rheumatol. 2003. 17:877–907.10. Israeli E, Agmon-Levin N, Blank M, Shoenfeld Y. Macrophagic myofaciitis a vaccine (alum) autoimmune-related disease. Clin Rev Allergy Immunol. 2011. 41:163–168.11. Chérin P, Menard D, Mouton P, Viallard JF, Le Hello C, Authier FJ, et al. Macrophagic myofasciitis associated with inclusion body myositis: a report of three cases. Neuromuscul Disord. 2001. 11:452–457.12. Schonberger LB, Bregman DJ, Sullivan-Bolyai JZ, Keenlyside RA, Ziegler DW, Retailliau HF, et al. Guillain-Barre syndrome following vaccination in the National Influenza Immunization Program, United States, 1976-1977. Am J Epidemiol. 1979. 110:105–123.13. Geier DA, Geier MR. A case-control study of serious autoimmune adverse events following hepatitis B immunization. Autoimmunity. 2005. 38:295–301.14. Verstraeten T, Descamps D, David MP, Zahaf T, Hardt K, Izurieta P, et al. Analysis of adverse events of potential autoimmune aetiology in a large integrated safety database of AS04 adjuvanted vaccines. Vaccine. 2008. 26:6630–6638.15. Orbach H, Agmon-Levin N, Zandman-Goddard G. Vaccines and autoimmune diseases of the adult. Discov Med. 2010. 9:90–97.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent focal myofasciitis of Behçet syndrome mimics infectious myofasciitis: a case report
- FDG-PET/CT Brain Findings in a Patient With Macrophagic Myofasciitis
- A Case of Sarcoidosis Presented with Myofasciitis
- Metastatic Carcinoma Manifesting as Clubbed Finger in a Patient with Lung Cancer
- A Case of the Bilateral Metastatic Endophthalmitis
