Korean Circ J.
2012 Jun;42(6):427-430. 10.4070/kcj.2012.42.6.427.
Cardiogenic Shock From Global Myocardial Ischemia Induced by Simultaneous Multivessel Coronary Spasm
- Affiliations
-
- 1Department of Internal Medicine, Dong-A University School of Medicine, Busan, Korea. kimyd@mail.donga.ac.kr
- KMID: 1433864
- DOI: http://doi.org/10.4070/kcj.2012.42.6.427
Abstract
- Coronary artery spasm is an uncommon, but well recognized, etiology for acute myocardial infarction. However, cardiogenic shock with myocardial infarction resulting from simultaneous multiple coronary artery spasm has been rarely reported, and not in Korea. Recently, we experienced such a case in a 50-year-old Korean man without previous diagnosis of variant angina. The patient, hospitalized for blood sugar control, developed severe chest pain accompanying ST-segment elevation in multiple leads. The patient immediately received cardiac catheterization because of cardiogenic shock. Coronary angiogram revealed the severe and simultaneous spasm of three major epicardial arteries, which was promptly relieved by an intracoronary administration of isosorbide dinitrate. This case highlights the need to rule out the potential mechanism of coronary spasm even in the most severe episodes of acute coronary syndrome.
MeSH Terms
Figure
-

Fig. 1 Result of electrocardiograms. A: electrocardiogram demonstrating ST-segment elevation in multiple leads and wide QRS widening with right bundle branch block morphology. B: electrocardiogram taken on arrival in the catherization room, showing ventricular fibrillation.
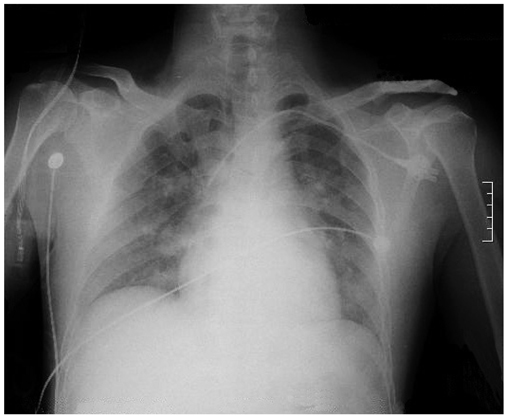
Fig. 2 Chest radiogram showing sign of pulmonary edema.
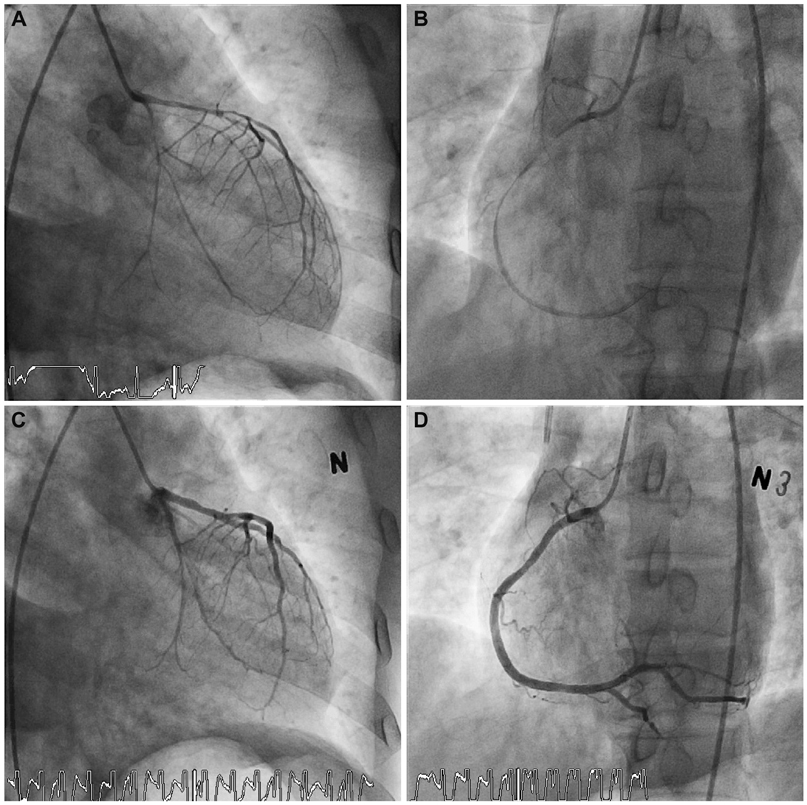
Fig. 3 Results of coronary angiogram. A and B: coronary angiogram showing widespread spasm of the left circumflex artery and left anterior descending artery (A) and right coronary artery (B). C and D: coronary angiogram after intracoronary administration of isosorbide dinitrate showing prompt relief of vasospam in all three coronary arteries.
Reference
-
1. Lange RL, Reid MS, Tresch DD, Keelan MH, Bernhard VM, Coolidge G. Nonatheromatous ischemic heart disease following withdrawal from chronic industrial nitroglycerin exposure. Circulation. 1972. 46:666–678.2. Severi S, Davies G, Maseri A, Marzullo P, L'Abbate A. Long-term prognosis of "variant" angina with medical treatment. Am J Cardiol. 1980. 46:226–232.3. Waters DD, Szlachcic J, Miller D, Theroux P. Clinical characteristics of pa-tients with variant angina complicated by myocardial infarction or death within 1 month. Am J Cardiol. 1982. 49:658–664.4. Waters DD, Miller D, Szlachcic J, et al. Factors influencing the long-term prognosis of treated patients with variant angina. Circulation. 1983. 68:258–265.5. Mark DB, Califf RM, Morris KG, et al. Clinical characteristics and long-term survival of patients with variant angina. Circulation. 1984. 69:880–888.6. Jeoung JY, Lim DS, Kang JA, et al. The study of coronary spasm by follow-up coronary angiography in variant angina. Korean Circ J. 2002. 32:791–797.7. Doo YC, Kim JS, Chae KS, et al. Clinical and angiographic characteristics and long-term follow-up in patients with variant angina who presented as acute myocardial infarction. Korean Circ J. 1999. 29:276–284.8. Leary T. Coronary spasm as a possible factor in producing sudden death. Am Heart J. 1935. 10:338–344.9. Saito H, Itoh T, Itoh M, Kanaya Y, Suzuki T, Hiramori K. Simultaneous mul-tivessel coronary spasm causing acute myocardial infarction: a case report. Angiology. 2007. 58:112–117.10. Vincent GM, Anderson JL, Marshall HW. Coronary spasm producing coronary thrombosis and myocardial infarction. N Engl J Med. 1983. 309:220–223.11. Meisel SR, Mazur A, Chetboun I, et al. Usefulness of implantable cardioverter-defibrillators in refractory variant angina pectoris complicated by ventricular fibrillation in patients with angiographically normal coronary arteries. Am J Cardiol. 2002. 89:1114–1116.12. Golzio PG, Orzan F, Ferrero P, et al. Myocardial infarction with normal coronary arteries: ten-year follow-up. Ital Heart J. 2004. 5:732–738.13. Da Costa A, Isaaz K, Faure E, Mourot S, Cerisier A, Lamaud M. Clinical characteristics, aetiological factors and long-term prognosis of myocardial infarction with an absolutely normal coronary angiogram; a 3-year follow-up study of 91 patients. Eur Heart J. 2001. 22:1459–1465.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Simultaneous acute myocardial infarction in two coronary arteries
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Coronary Intervention of Cardiogenic Shock in Acute Myocardial Infarction
- Cardiogenic Shock in a Patient with Intermediate Coronary Artery Disease due to Preoperative Spasm
- Acute Myocardial Infarction with Simultaneous Occlusions of Left Anterior Descending Artery and Right Coronary Artery
