J Korean Fract Soc.
2013 Jan;26(1):60-64. 10.12671/jkfs.2013.26.1.60.
Costoclavicular Syndrome Secondary to Nonunion of a Displaced Fracture of the Clavicle, Misdiagnosed as a Simple Muscle Strain: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, Sung-Ae Hospital, Seoul, Korea. jsj232@naver.com
- 2Department of Orthopaedic Surgery, Gwangmyeong Sung-Ae Hospital, Gwangmyeong, Korea.
- KMID: 1431719
- DOI: http://doi.org/10.12671/jkfs.2013.26.1.60
Abstract
- Thoracic outlet syndrome is a relatively common disease. However, costoclavicular syndrome as a condition secondary to nonunion of a displaced fracture of the clavicle is very rare. Most clavicular fractures in adults are united with no or minimal persistent symptoms. Also, symptomatic nonunion of a displaced fracture of the clavicle is rare. A 55-year-old male initially presented with persistent forearm pain after slip-down was initially diagnosed with simple muscle strain. However, he was given a delayed diagnosis of costoclavicular syndrome, caused by compression of the subclavian artery due to trauma in the fibrotic nonunion of the right clavicle without apparent symptoms. We obtained satisfactory results by surgical treatment. Here we report this case with a review of the literature.
MeSH Terms
Figure
-

Fig. 1 Preoperative radiograph shows a fibrous nonunion and displacement with shortening of the clavicle shaft.

Fig. 2 Preoperative 3dimension computed tomography shows displacement and shortening of the clavicle shaft.
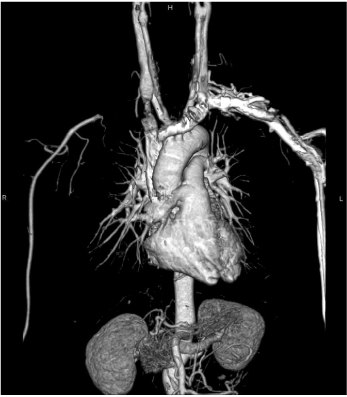
Fig. 3 Preoperative angio computed tomography shows the discontinuous subclavian artery under the fracture site.
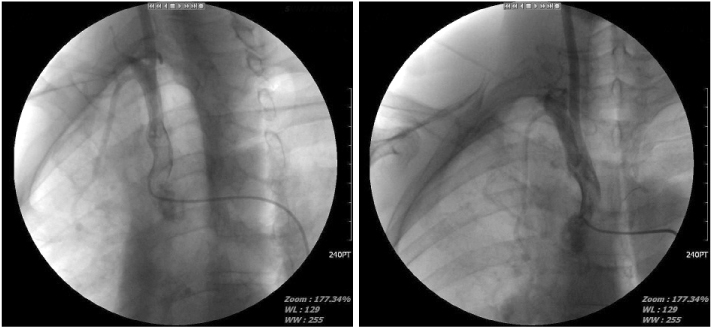
Fig. 4 Preoperative angiogram shows the discontinuous subclavian artery beneath the fracture site with little collateral circulation.
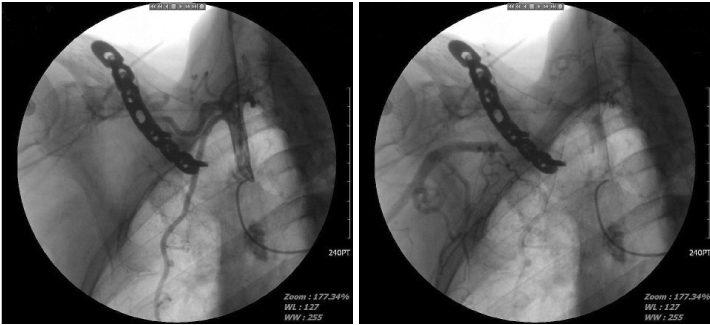
Fig. 5 Postoperative angiogram shows restoration of circulation at the brachial artery, distal to the fracture site.

Fig. 6 Postoperative radiograph shows the union of the fracture site with no displacement.
Reference
-
1. Davidovic LB, Kostic DM, Jakovljevic NS, Kuzmanovic IL, Simic TM. Vascular thoracic outlet syndrome. World J Surg. 2003. 27:545–550.
Article2. Garnier D, Chevalier J, Ducasse E, Modine T, Espagne P, Puppinck P. Arterial complications of thoracic outlet syndrome and pseudarthrosis of the clavicle: three patients. J Mal Vasc. 2003. 28:79–84.3. Hahn SB, Park BM, Lim YJ. Thoracic outlet syndrome. J Korean Orthop Assoc. 1990. 25:919–926.
Article4. Lee YM, Song SW, Choi KB, Rhee SK. The treatment of thoracic outlet syndrome. J Korean Soc Microsurg. 2011. 20:102–107.5. Mulder DS, Greenwood FA, Brooks CE. Posttraumatic thoracic outlet syndrome. J Trauma. 1973. 13:706–715.
Article6. Patterson RH. Cervical ribs and the scalenus muscle syndrome. Ann Surg. 1940. 111:531–545.
Article7. Roos DB. The thoracic outlet syndrome is underrated. Arch Neurol. 1990. 47:327–328.
Article8. Sohn SK, Kim SS, Song CG, Kwak JI. Costoclavicular syndrome: a case report. J Korean Fract Soc. 2007. 20:86–89.
Article9. Tindall SC. Youmans JR, editor. Chronic injuries of peripheral nerves by entrapment. Neurological surgery. 1996. 4th ed. Philadelphia: WB Saunders Co;2182–2187.10. Wilbourn AJ. The thoracic outlet syndrome is overdiagnosed. Arch Neurol. 1990. 47:328–330.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Costoclavicular Syndrome: A Case Report
- Infected Nonunion of Clavicle Shaft after Operation: A Case Report
- Progressive Brachial Plexus Palsy after Fixation of Clavicle Shaft Nonunion: A Case Report
- Operative Treatment of the Displaced Clavicle Shaft Fracture in Adult
- Delayed subclavian - Vein thrombosis Following Nonunion of the Clavicular Fracture: A Case Report
