Mesenteric Vascular Occlusion: Comparison of Ancillary CT Findings between Arterial and Venous Occlusions and Independent CT Findings Suggesting Life-Threatening Events
- Affiliations
-
- 1Division of Emergency and Critical Care Radiology, Department of Medical Imaging and Intervention, Chang Gung Memorial Hospital, Chang Gung University, Taoyuan 333, Taiwan. ycwong@adm.cgmh.org.tw
- 2Division of Trauma and Emergency, Department of Surgery, Chang Gung Memorial Hospital, Chang Gung University, Taoyuan 333, Taiwan.
- KMID: 1430042
- DOI: http://doi.org/10.3348/kjr.2013.14.1.38
Abstract
OBJECTIVE
To compare the ancillary CT findings between superior mesenteric artery thromboembolism (SMAT) and superior mesenteric vein thrombosis (SMVT), and to determine the independent CT findings of life-threatening mesenteric occlusion.
MATERIALS AND METHODS
Our study was approved by the institution review board. We included 43 patients (21 SMAT and 22 SMVT between 1999 and 2008) of their median age of 60.0 years, and retrospectively analyzed their CT scans. Medical records were reviewed for demographics, management, surgical pathology diagnosis, and outcome. We compared CT findings between SMAT and SMVT groups. Multivariate analysis was conducted to determine the independent CT findings of life-threatening mesenteric occlusion.
RESULTS
Of 43 patients, 24 had life-threatening mesenteric occlusion. Death related to mesenteric occlusion was 32.6%. A thick bowel wall (p < 0.001), mesenteric edema (p < 0.001), and ascites (p = 0.009) were more frequently associated with SMVT, whereas diminished bowel enhancement (p = 0.003) and paralytic ileus (p = 0.039) were more frequent in SMAT. Diminished bowel enhancement (OR = 20; p = 0.007) and paralytic ileus (OR = 16; p = 0.033) were independent findings suggesting life-threatening mesenteric occlusion.
CONCLUSION
The ancillary CT findings occur with different frequencies in SMAT and SMVT. However, the independent findings indicating life-threatening mesenteric occlusion are diminished bowel wall enhancement and paralytic ileus.
Keyword
MeSH Terms
Figure
-

Fig. 1 46 year-old male of nephrotic syndrome. CT scans shows acute superior mesenteric vein thrombosis (black arrow) with bowel wall thickening (white arrowhead), mesenteric edema (black arrowhead) and ascites. Note the normal SMA enhancement (white arrow) and ratio of SMV to SMA diameters > 2. He did not receive surgery but was treated with anticoagulation therapy. Follow-up CT showed abundant collateral veins and no bowel necrosis. SMA = superior mesenteric artery, SMV = superior mesenteric vein
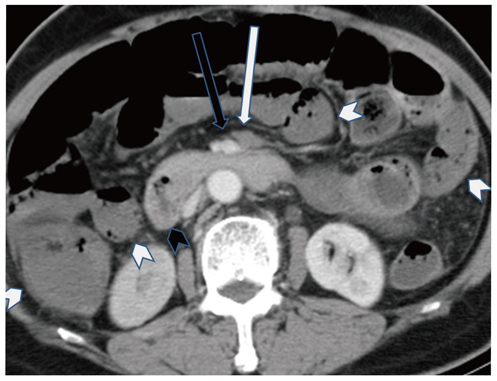
Fig. 2 73 year-old female of atrial fibrillation and paralytic ileus. CT scan shows acute superior mesenteric artery occlusion (white arrow) with diminished enhancement of thin bowel walls (white arrowheads) as compared to normal duodenum (black arrowhead). Note normal SMV enhancement (black arrow) and ratio of SMV to SMA diameters of about 1. Extensive bowel gangrene was found at exploratory laparotomy. Bowel resection was not possible and she died of sepsis and acidosis. SMA = superior mesenteric artery, SMV = superior mesenteric vein
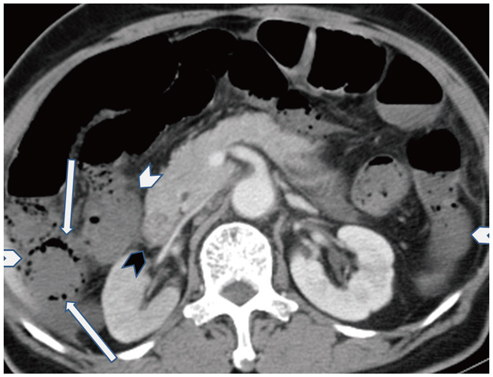
Fig. 3 Although the SMA orifice is normally enhanced, CT scans caudal to this level (not shown) reveal acute superior mesenteric artery occlusion. Note diminished enhancement of thin bowel walls (white arrowheads) as compared to normal duodenum (black arrowhead) and pneumatosis intestinalis (white arrows). Resection of small bowel and right colon showed coagulative necrosis. This 86 year-old female patient died of sepsis 4 days later. SMA = superior mesenteric artery
Reference
-
1. Schoots IG, Koffeman GI, Legemate DA, Levi M, van Gulik TM. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. Br J Surg. 2004. 91:17–27.2. Yasuhara H. Acute mesenteric ischemia: the challenge of gastroenterology. Surg Today. 2005. 35:185–195.3. Martinez JP, Hogan GJ. Mesenteric ischemia. Emerg Med Clin North Am. 2004. 22:909–928.4. Bakal CW, Sprayregen S, Wolf EL. Radiology in intestinal ischemia. Angiographic diagnosis and management. Surg Clin North Am. 1992. 72:125–141.5. Klein HM, Lensing R, Klosterhalfen B, Töns C, Günther RW. Diagnostic imaging of mesenteric infarction. Radiology. 1995. 197:79–82.6. Kim JH, Ha HK, Sohn MJ, Shin BS, Lee YS, Chung SY, et al. Usefulness of MR imaging for diseases of the small intestine: comparison with CT. Korean J Radiol. 2000. 1:43–50.7. Leschka S, Alkadhi H, Wildermuth S, Marincek B. Multi-detector computed tomography of acute abdomen. Eur Radiol. 2005. 15:2435–2447.8. Federle MP. CT of the acute (emergency) abdomen. Eur Radiol. 2005. 15:Suppl 4. D100–D104.9. Horton KM, Fishman EK. Multi-detector row CT of mesenteric ischemia: can it be done? Radiographics. 2001. 21:1463–1473.10. Rosow DE, Sahani D, Strobel O, Kalva S, Mino-Kenudson M, Holalkere NS, et al. Imaging of acute mesenteric ischemia using multidetector CT and CT angiography in a porcine model. J Gastrointest Surg. 2005. 9:1262–1274. discussion 1274-1275.11. Kirkpatrick ID, Kroeker MA, Greenberg HM. Biphasic CT with mesenteric CT angiography in the evaluation of acute mesenteric ischemia: initial experience. Radiology. 2003. 229:91–98.12. Wiesner W, Khurana B, Ji H, Ros PR. CT of acute bowel ischemia. Radiology. 2003. 226:635–650.13. Segatto E, Mortelé KJ, Ji H, Wiesner W, Ros PR. Acute small bowel ischemia: CT imaging findings. Semin Ultrasound CT MR. 2003. 24:364–376.14. Romano S, Romano L, Grassi R. Multidetector row computed tomography findings from ischemia to infarction of the large bowel. Eur J Radiol. 2007. 61:433–441.15. Tang ZH, Qiang JW, Feng XY, Li RK, Sun RX, Ye XG. Acute mesenteric ischemia induced by ligation of porcine superior mesenteric vein: multidetector CT evaluations. Acad Radiol. 2010. 17:1146–1152.16. Rha SE, Ha HK, Lee SH, Kim JH, Kim JK, Kim JH, et al. CT and MR imaging findings of bowel ischemia from various primary causes. Radiographics. 2000. 20:29–42.17. Moschetta M, Stabile Ianora AA, Pedote P, Scardapane A, Angelelli G. Prognostic value of multidetector computed tomography in bowel infarction. Radiol Med. 2009. 114:780–791.18. Chang RW, Chang JB, Longo WE. Update in management of mesenteric ischemia. World J Gastroenterol. 2006. 12:3243–3247.19. Gore RM, Yaghmai V, Thakrar KH, Berlin JW, Mehta UK, Newmark GM, et al. Imaging in intestinal ischemic disorders. Radiol Clin North Am. 2008. 46:845–875. v20. Romano S, Niola R, Maglione F, Romano L. Small bowel vascular disorders from arterial etiology and impaired venous drainage. Radiol Clin North Am. 2008. 46:891–908. vi21. Romano S, Lassandro F, Scaglione M, Romano L, Rotondo A, Grassi R. Ischemia and infarction of the small bowel and colon: spectrum of imaging findings. Abdom Imaging. 2006. 31:277–292.22. Chou CK, Wu RH, Mak CW, Lin MP. Clinical significance of poor CT enhancement of the thickened small-bowel wall in patients with acute abdominal pain. AJR Am J Roentgenol. 2006. 186:491–498.23. Cenedese A, Monneuse O, Gruner L, Tissot E, Mennesson N, Barth X. Initial management of extensive mesenteric venous thrombosis: retrospective study of nine cases. World J Surg. 2009. 33:2203–2208.24. Kurimoto Y, Morishita K, Fukada J, Kawaharada N, Komatsu K, Yama N, et al. A simple but useful method of screening for mesenteric ischemia secondary to acute aortic dissection. Surgery. 2004. 136:42–46.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Helical CT Findings in Mesenteric Ischemia
- A novel hybrid technique to treat flush mesenteric arterial occlusion in acute-on-chronic mesenteric ischemia
- Radiological Findings of Vascular Involvement in Behcet's Disease
- Two Cases of Acute Mesenteric Infarction Due to Superior Mesenteric Arterial and Venous Branch Occlusion
- Assessment of Mesenteric Vascular Steno-occlusive Lesion in Acute Mesenteric Ischemia: Comparison between CT Angiography and Digital Subtraction Angiography
