Korean J Neurotrauma.
2012 Apr;8(1):15-20. 10.13004/kjnt.2012.8.1.15.
The Differences of Radiological Results after Percutaneous Vertebroplasty according to the Degree of Preoperative Canal Encroachment due to Bony Fragments
- Affiliations
-
- 1Department of Neurosurgery, Seoul Veterans Hospital, Seoul, Korea. euro3399@naver.com
- KMID: 1427677
- DOI: http://doi.org/10.13004/kjnt.2012.8.1.15
Abstract
OBJECTIVE
Anterior wedge compression fractures and burst fractures have different clinical features, treatment methods and risks of neurologic deficits. The aim of this study was to evaluate the radiological differences and postoperative risk due to cement leakage after vertebroplasty.
METHODS
From January 2007 to December 2008, we retrospectively analyzed the radiological features of 43 patients. We divided the patients into three groups by the degree of the displaced bony fragments into the spinal canal. The change of the compression ratio, the kyphotic angle, the presence of cement leakage and the occurrence of major complications were investigated.
RESULTS
The immediately postoperative improvement of the compression ratio was significantly better in the anterior wedge compression fracture group than that in the burst compression group (p-value: 0.022). Cement leakage was more common in the burst fracture group even though this was not statistically significant (p-value: 0.114), but cement leakage into spinal canal did not occur. There was no major complication, including embolism and additional neurologic deficit, after vertebroplasty in all the patients.
CONCLUSION
Vertebroplasty was the more effective method for treating an anterior wedge fracture than a burst fracture, and especially for achieving an improved compression ratio. Even though the risk of cement leakage may be higher for a burst fracture, vertebroplasty may be also carefully applied to burst fracture patients with no neurologic deficits at admission.
MeSH Terms
Figure
-

FIGURE 1. Preoperative lumbar CT shows the degree of canal encroachment due to bony fragment. None (A), less than 20% (B), more than 20% (C).
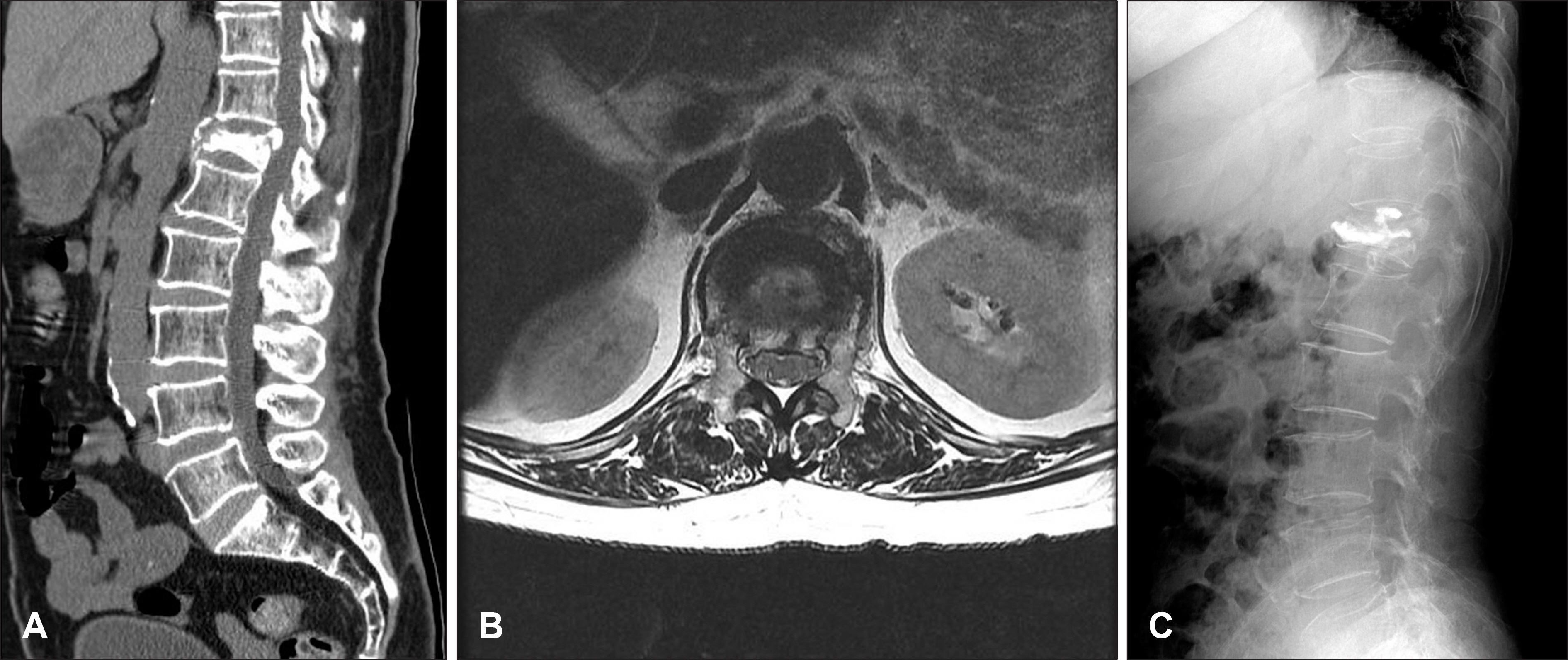
FIGURE 2. Preoperative lumbar CT and axial MRI image shows canal encroachment more than 20% (A, B). Simple X-ray lateral view after vertebroplasty (C).
Reference
-
1). Amoretti N., Hovorka E., Marcy PY., Lamasse C., Brunner P., Roux C, et al. Burst fracture of the spine involving vertebrae presenting no other lesions: the role of vertebroplasty. Clin Imaging. 29:379–382. 2005.2). Appel NB., Gilula LA. Percutaneous vertebroplasty in patients with spinal canal compromise. AJR Am J Roentgenol. 182:947–951. 2004.
Article3). Chow GH., Nelson BJ., Gebhard JS., Brugman JL., Brown CW., Donaldson DH. Functional outcome of thoracolumbar burst fractures managed with hyperextension casting or bracing and early mobilization. Spine (Phila Pa 1976). 21:2170–2175. 1996.
Article4). Dai LY., Jiang SD., Wang XY., Jiang LS. A review of the management of thoracolumbar burst fractures. Surg Neurol. 67:221–231. discussion 231. 2007.
Article5). Dai LY., Wang XY., Jiang LS. Evaluation of traumatic spinal canal stenosis in thoracolumbar burst fractures. A comparison of three methods for measuring the percent canal occlusion. Eur J Radiol. 67:526–530. 2008.6). Doody O., Czarnecki C., Given MF., Lyon SM. Vertebroplasty in the management of traumatic burst fractures: a case series. J Med Imaging Radiat Oncol. 53:489–492. 2009.
Article7). Esses SI., Botsford DJ., Kostuik JP. Evaluation of surgical treatment for burst fractures. Spine (Phila Pa 1976). 15:667–673. 1990.
Article8). Frank E., Bonsell S. The accuracy of anterior-posterior measurements in the assessment of spinal canal compromise in burst fractures. Neurol Res. 16:410–412. 1994.
Article9). Hashimoto T., Kaneda K., Abumi K. Relationship between traumatic spinal canal stenosis and neurologic deficits in thoracolumbar burst fractures. Spine (Phila Pa 1976). 13:1268–1272. 1988.
Article10). Hiwatashi A., Westesson PL. Vertebroplasty for osteoporotic fractures with spinal canal compromise. AJNR Am J Neuroradiol. 28:690–692. 2007.11). Knight RQ., Stornelli DP., Chan DP., Devanny JR., Jackson KV. Comparison of operative versus nonoperative treatment of lumbar burst fractures. Clin Orthop Relat Res. 293:112–121. 1993.
Article12). Leferink VJ., Nijboer JM., Zimmerman KW., Veldhuis EF., ten Vergert EM., ten Duis HJ. Burst fractures of the thoracolumbar spine: changes of the spinal canal during operative treatment and follow-up. Eur Spine J. 12:255–260. 2003.
Article13). Li CH., Chang MC., Liu CL., Chen TS. Osteoporotic burst fracture with spinal canal compromise treated with percutaneous vertebroplasty. Clin Neurol Neurosurg. 112:678–681. 2010.
Article14). Meves R., Avanzi O. Correlation between neurological deficit and spinal canal compromise in 198 patients with thoracolumbar and lumbar fractures. Spine (Phila Pa 1976). 30:787–791. 2005.
Article15). Mumford J., Weinstein JN., Spratt KF., Goel VK. Thoracolumbar burst fractures. The clinical efficacy and outcome of nonoperative management. Spine (Phila Pa 1976). 18:955–970. 1993.16). Noh CH., Yi JS., Lee HJ., Yang JH., Lee IW., Kim MC. Effect of percutaneous vertebroplasty with polymethylmethacrylate to osteoporotic spinal compression fractures and bursting fractures. J Korean Neurosurg Soc. 35:365–371. 2004.17). Patel AA., Vaccaro AR., Martyak GG., Harrop JS., Albert TJ., Ludwig SC, et al. Neurologic deficit following percutaneous vertebral stabilization. Spine (Phila Pa 1976). 32:1728–1734. 2007.
Article18). Schnee CL., Ansell LV. Selection criteria and outcome of operative approaches for thoracolumbar burst fractures with and without neurological deficit. J Neurosurg. 86:48–55. 1997.
Article19). Shen WJ., Shen YS. Nonsurgical treatment of three-column thoracolumbar junction burst fractures without neurologic deficit. Spine (Phila Pa 1976). 24:412–415. 1999.
Article20). Shin JJ., Chin DK., Yoon YS. Percutaneous vertebroplasty for the treatment of osteoporotic burst fractures. Acta Neurochir (Wien). 151:141–148. 2009.
Article21). Tropiano P., Huang RC., Louis CA., Poitout DG., Louis RP. Functional and radiographic outcome of thoracolumbar and lumbar burst fractures managed by closed orthopaedic reduction and casting. Spine (Phila Pa 1976). 28:2459–2465. 2003.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preliminary Report of Percutaneous Vertebroplasty for the Treatment of the Burst Fractures with Spinal Canal Encroachment
- Relationship between Simple X-ray and CT Findings on the Degree of Canal Encroachment in Burst Fracture of Thoracolumbar Junction
- Spinal Canal Remodelling after Stabilization of Thoracolumbar Burst Fractures
- Lumbar Root Injury by the Leakage of Bone Cement after the Percutaneous Vertebroplasty: A case report
- The Effect of Pedicle Screw Instrumentation on Fractured Vertebrae in Unstable Thoracolumbar Burst Fractures with Canal Encroachment and Clinical Result
