Characteristic MRI Findings of Spinal Metastases from Various Primary Cancers: Retrospective Study of Pathologically-Confirmed Cases
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul, Korea. hotsong@yuhs.ac
- KMID: 1426746
- DOI: http://doi.org/10.13104/jksmrm.2013.17.1.8
Abstract
- PURPOSE
The purpose of this study was to find and categorize the various magnetic resonance imaging (MRI) findings of spinal metastases that correlate with the type of primary cancer.
MATERIALS AND METHODS
We retrospectively reviewed gadolinium-enhanced magnetic resonance images of 30 patients with 169 spinal metastatic lesions from lung cancer (n = 56), breast cancer (n = 29), colorectal cancer (n = 20), hepatocellular carcinoma (HCC) (n = 17), and stomach cancer (n = 47). The size, location, extent of invasion, signal intensity, margin, enhancement pattern, and osteoblastic or osteolytic characteristics of each metastatic tumor were analyzed.
RESULTS
The metastatic lesions from HCC were larger than those from the other primary tumors (P < 0.05) except for colorectal cancer (P = 0.268). Well-defined metastatic tumor margins were more frequently seen in lung cancer and breast cancer (P < 0.01). All but HCC showed a tendency to invade the vertebral body rather than the posterior elements (P < 0.02). Colorectal cancer and HCC showed a tendency toward extraosseous invasion without statistical significance. HCC showed a characteristic enhancement pattern of 'worms-in-a-bag'. Rim enhancement with a sclerotic center was only seen in spinal metastases from stomach cancer.
CONCLUSION
Despite many overlapping imaging features, spinal metastases of various primary tumors display some characteristic MRI findings that can help identify the primary cancer.
Keyword
MeSH Terms
Figure
-
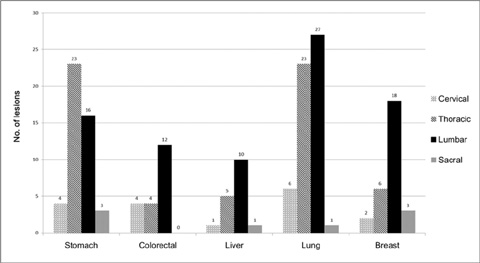
Fig. 1 Vertebral levels of spinal metastasis according to the origin of primary cancer.
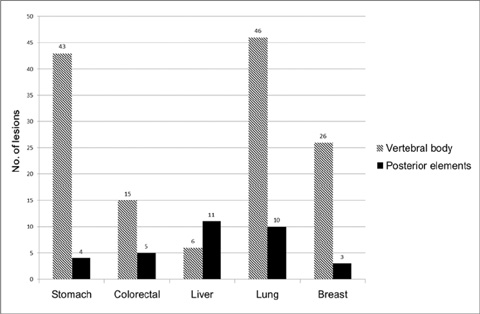
Fig. 2 Predilection for sites of metastasis according to the five different types of primary cancer.
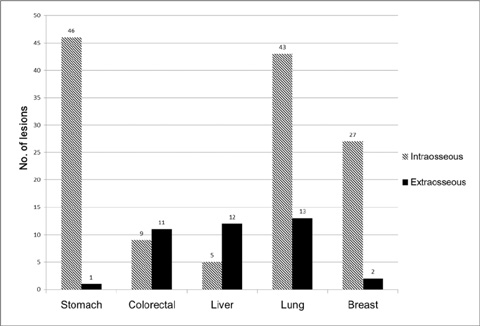
Fig. 3 Tendency toward intra- or extraosseous invasion of spinal metastasis according to the five different types of primary cancer.
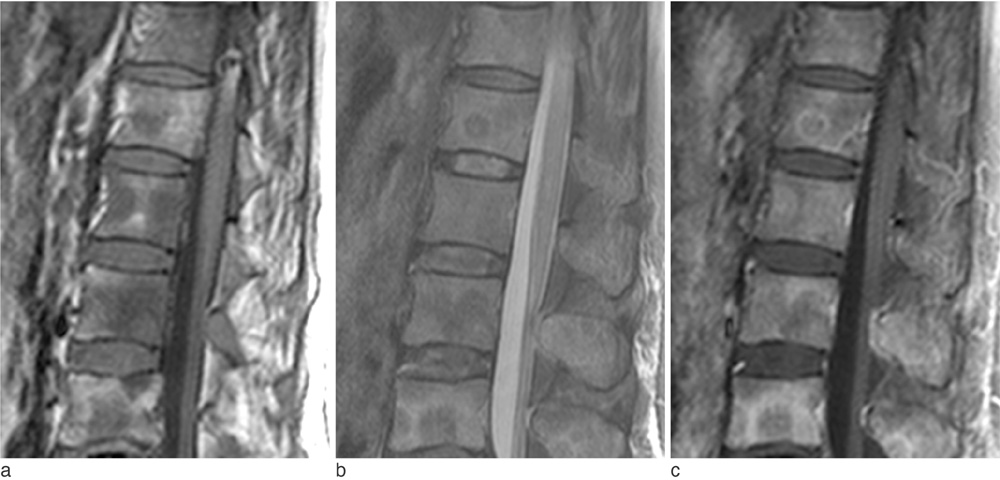
Fig. 4 A 60-year-old woman with advanced gastric cancer. a. T1-weighted sagittal image of the thoracolumbar spine showing multiple hypointense metastatic lesions. b. On fat-suppressed T2-weighted sagittal image, the lesions show hyperintensity in the periphery but hypointensity in the center, which may indicate sclerotic changes in the center of the metastatic lesions. c. Contrast-enhanced T1-weighted sagittal image with fat suppression demonstrates enhancement in the periphery of the lesions as well as involvement of the bone marrow.
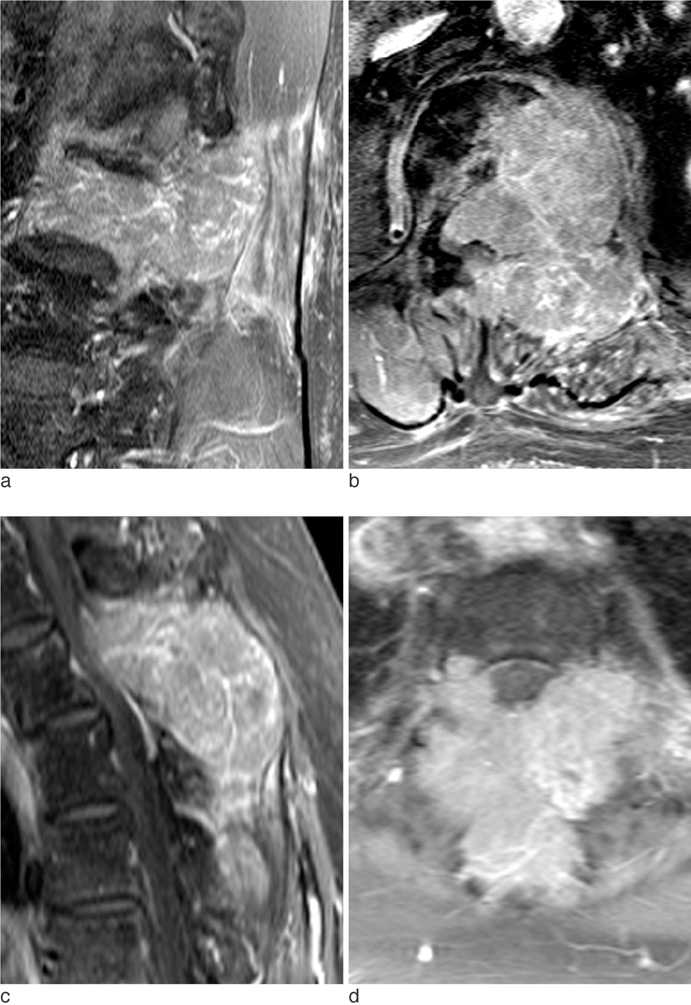
Fig. 5 Two patients with spine metastases from hepatocellular carcinoma. a, b. Contrast-enhanced T1-weighted sagittal (a) and axial (b) images with fat-suppression of the lumbar spine of a 62-year-old man. A large expansile well-enhancing mass is invading the vertebral body and adjacent structures posteriorly, causing central canal obstruction. Note many curvilinear structures showing strong enhancement within the tumor ('worms-in-a-bag' enhancement pattern). c, d. Contrast-enhanced T1-weighted sagittal (c) and axial (d) images with fatsuppression of the cervical spine of a 69-year-old woman. The location, extent of disease, and enhancement pattern are almost the same as those seen in the patient in a, b.
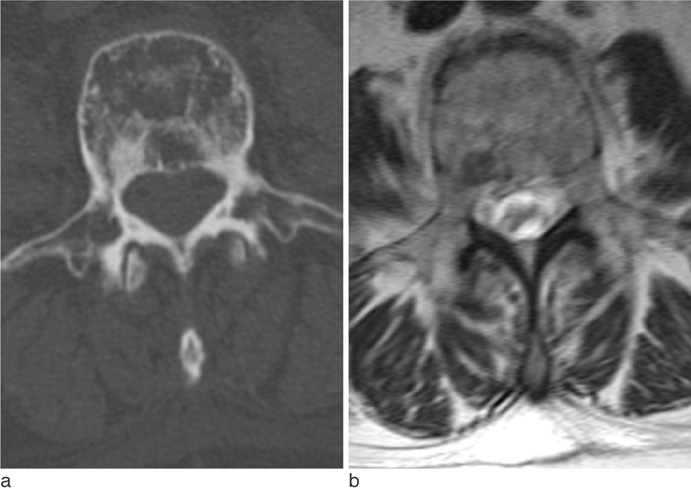
Fig. 6 A 56-year-old woman with spine metastases from breast cancer. a. CT axial image shows mixed osteolytic and osteoblastic areas in the vertebra. b. Corresponding T2-weighted axial image of the same level clearly demonstrates that sclerotic areas show hypointensity while osteolytic areas show hyperintensity on T2-weighted MRI.

Fig. 7 Mass formation from spinal metastases of three different primary tumors. a. A 76-year-old man with lung cancer. Contrast-enhanced T1-weighted sagittal image shows a homogeneously-enhancing metastatic mass replacing the 5th lumbar vertebra and spreading beneath the anterior longitudinal ligament upward. b. A 74-year-old man with colorectal cancer. On contrast-enhanced T1-weighted sagittal image of the cervical spine, a heterogeneously-enhancing metastatic mass involving two vertebrae extends anteriorly to form a bulging mass. c. A 69-year-old woman with HCC (same patient as in Fig. 5c). On contrast-enhanced T1-weighted sagittal image, a huge hypervascular mass invades the posterior aspect of the cervical spine. Note the 'worms-in-a-bag' enhancement pattern.
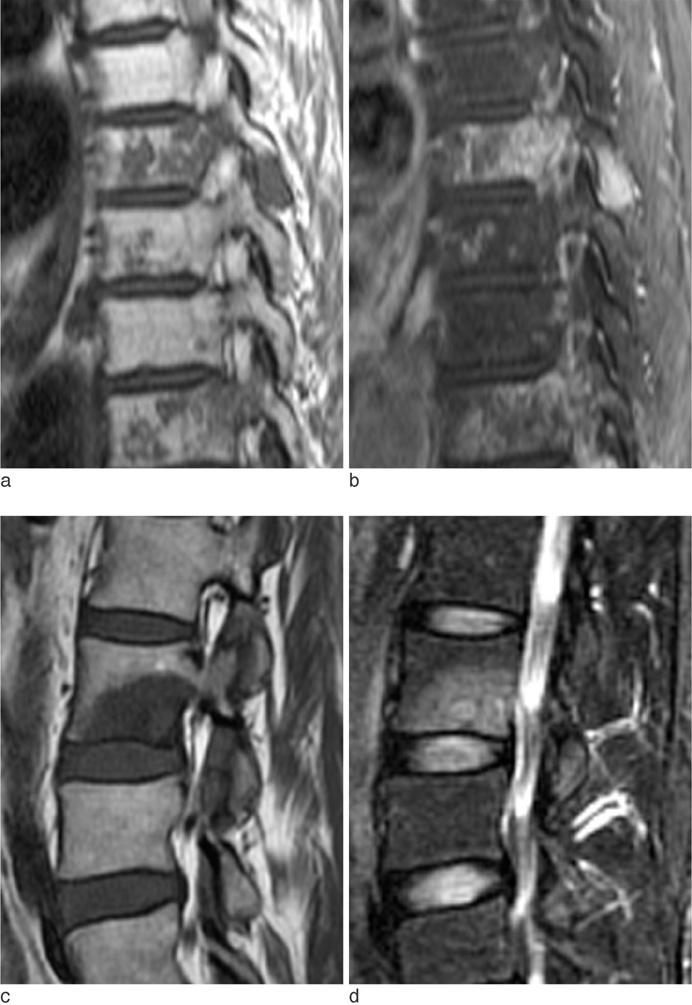
Fig. 8 Metastatic lesions confined to the vertebrae. a, b. Pre-contrast (a) and contrastenhanced with fat suppression (b) T1-weighted sagittal images of a 56-yearold woman with lung cancer. There are numerous well-defined hypointense lesions with non-specific heterogeneous contrast enhancement in the thoracic spine. These lesions are confined in the vertebrae, some of which appear to coalesce. c, d. T1-weighted (c) and T2-weighted with fat suppression (d) sagittal images of a 45-year-old woman with breast cancer. There is a well-defined hypointense metastatic lesion with homogeneous enhancement in the lumbar vertebra. This lesion is also confined in the vertebral body without extraosseous invasion, despite its relatively large size.
Reference
-
1. Boland PJ, Lane JM, Sundaresan N. Metastatic disease of the spine. Clin Orthop Relat Res. 1982; 169:95–102.2. Schiff D, O'Neill BP, Suman VJ. Spinal epidural metastasis as the initial manifestation of malignancy: clinical features and diagnostic approach. Neurology. 1997; 49:452–456.3. Berrettoni BA, Carter JR. Mechanisms of cancer metastasis to bone. J Bone Joint Surg Am. 1986; 68:308–312.4. Guillevin R, Vallee JN, Lafitte F, Menuel C, Duverneuil NM, Chiras J. Spine metastasis imaging: review of the literature. J Neuroradiol. 2007; 34:311–321.5. Daugaard G. Unknown primary tumours. Cancer Treat Rev. 1994; 20:119–147.6. Abbruzzese JL, Abbruzzese MC, Hess KR, Raber MN, Lenzi R, Frost P. Unknown primary carcinoma: natural history and prognostic factors in 657 consecutive patients. J Clin Oncol. 1994; 12:1272–1280.7. Katagiri H, Takahashi M, Inagaki J, Sugiura H, Ito S, Iwata H. Determining the site of the primary cancer in patients with skeletal metastasis of unknown origin: a retrospective study. Cancer. 1999; 86:533–537.8. Brihaye J, Ectors P, Lemort M, Van Houtte P. The management of spinal epidural metastases. Adv Tech Stand Neurosurg. 1988; 16:121–176.9. Ghanem N, Uhl M, Brink I, et al. Diagnostic value of MRI in comparison to scintigraphy, PET, MS-CT and PET/CT for the detection of metastases of bone. Eur J Radiol. 2005; 55:41–55.10. Chiewvit P, Danchaivijitr N, Sirivitmaitrie K, Chiewvit S, Thephamongkhol K. Does magnetic resonance imaging give value-added than bone scintigraphy in the detection of vertebral metastasis? J Med Assoc Thai. 2009; 92:818–829.11. Beltran J, Noto AM, Chakeres DW, Christoforidis AJ. Tumors of the osseous spine: staging with MR imaging versus CT. Radiology. 1987; 162:565–569.12. Keogh C, Bergin D, Brennan D, Eustace S. MR imaging of bone tumors of the cervical spine. Magn Reson Imaging Clin N Am. 2000; 8:513–528.13. Ross JS, Moore KR, Borg B, Crim J, Shah LM. Diagnostic imaging: Spine. 2nd ed. Salt Lake City: Amirsys;2010.14. Sugimura K, Kajitani A, Okizuka H, Sugihara M, Mizutani M, Ishida T. Assessing response to therapy of spinal metastases with gadolinium-enhanced MR imaging. J Magn Reson Imaging. 1991; 1:481–484.15. Sneag DB, Krajewski K, Giardino A, et al. Extrahepatic spread of hepatocellular carcinoma: spectrum of imaging findings. AJR Am J Roentgenol. 2011; 197:W658–W664.16. Katyal S, Oliver JH 3rd, Peterson MS, Ferris JV, Carr BS, Baron RL. Extrahepatic metastases of hepatocellular carcinoma. Radiology. 2000; 216:698–703.17. Seo HJ, Choi YJ, Kim HJ, et al. Evaluation of bone metastasis from hepatocellular carcinoma using 18F-FDG PET/CT and 99mTc-HDP bone scintigraphy: characteristics of soft tissue formation. Nucl Med Mol Imaging. 2011; 45:203–211.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of Prognoses according to Breast MRI Results in Patients with Axillary Lymph Node Metastases from an Unknown Primary Origin
- MR Myelography
- Spinal Presentation of Spontaneous Intracranial Hypotension
- MR findings of spinal epidural mass
- Can Initial 18F-FDG PET-CT Imaging Give Information onMetastasis in Patients with Primary Renal Cell Carcinoma?
