J Korean Neurosurg Soc.
2013 Apr;53(4):252-254. 10.3340/jkns.2013.53.4.252.
A Textiloma on the Pterion : A Rarely Occurred Craniotomy Complication
- Affiliations
-
- 1Department of Neurosurgery, Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. bach1158@dsmc.or.kr
- KMID: 1426214
- DOI: http://doi.org/10.3340/jkns.2013.53.4.252
Abstract
- Textiloma is an inflammatory mass containing surgical sponges that are unintentionally left behind in a surgical wound. This complication has been most commonly described by abdominal and gynecologic surgeons. However, the occurrence of textiloma after intracranial procedures especially under the temporalis muscle has not been documented. The author reports a rare case of textiloma of the pterion in a patient who presented with a subcutaneous tumor developed eight years after frontotemporal craniotomy for aneurysm clipping.
Keyword
Figure
-
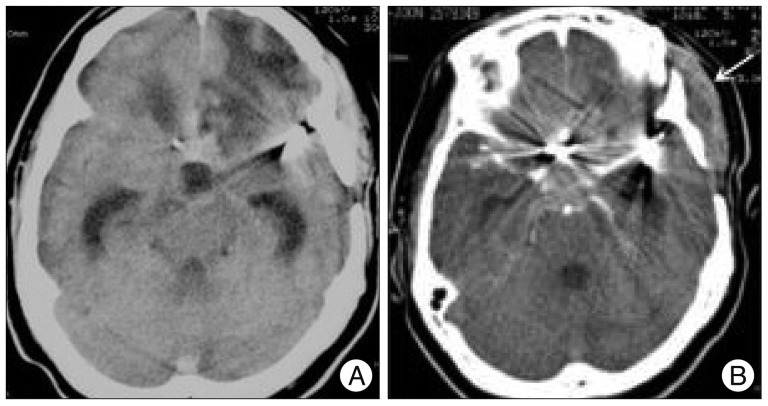
Fig. 1 Computed tomography of a textiloma developed after pterional craniotomy for aneurysm clipping. Nonenhanced (A) and enhanced (B) scans show an isodensity of homogeneous mass with a peripheral contrast enhancement in the temporalis muscle (arrow).
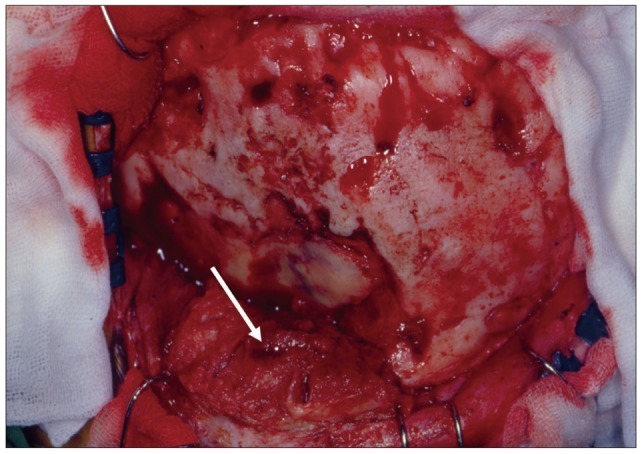
Fig. 2 Intraoperative appearance of the lesion demonstrates an osseous defect and a mass of granulation tissues adherent to the temporalis muscle (arrow). The lesion is extending into the underlying dura mater.

Fig. 3 Photomicrograph reveals gauze fibers (arrowhead) surrounded by dense fibrous connective tissue infiltrated with lymphocytes, plasma cells, neutrophilic granulocytes and macrophages (H&E, original magnification ×40).
Reference
-
1. Apel-Sarid L, Cochrane DD, Steinbok P, Byrne AT, Dunham C. Microfibrillar collagen hemostat-induced necrotizing granulomatous inflammation developing after craniotomy : a pediatric case series. J Neurosurg Pediatr. 2010; 6:385–392. PMID: 20887115.
Article2. Chen J, Lee S, Lui T, Yeh Y, Chen T, Tzaan W. Teflon granuloma after microvascular decompression for trigeminal neuralgia. Surg Neurol. 2000; 53:281–287. PMID: 10773262.
Article3. Cima RR, Kollengode A, Garnatz J, Storsveen A, Weisbrod C, Deschamps C. Incidence and characteristics of potential and actual retained foreign object events in surgical patients. J Am Coll Surg. 2008; 207:80–87. PMID: 18589366.
Article4. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003; 348:229–235. PMID: 12529464.
Article5. Goldsberry DH, Ross IB, Dhillon G, Corbett JJ. Visual dysfunction caused by gauze wrapping of an intracranial aneurysm. J Neuroophthalmol. 2004; 24:42–45. PMID: 15206439.
Article6. Kim AK, Lee EB, Bagley LJ, Loevner LA. Retained surgical sponges after craniotomies : imaging appearances and complications. AJNR Am J Neuroradiol. 2009; 30:1270–1272. PMID: 19213821.
Article7. Kucukyuruk B, Biceroglu H, Abuzayed B, Ulu MO, Kafadar AM. Paraspinal gossybipoma : a case report and review of the literature. J Neurosci Rural Pract. 2010; 1:102–104. PMID: 21808514.8. Manzella A, Filho PB, Albuquerque E, Farias F, Kaercher J. Imaging of gossypibomas : pictorial review. AJR Am J Roentgenol. 2009; 193(6 Suppl):S94–S101. PMID: 19933682.9. Vishteh AG, Apostolides PJ, Dean B, Spetzler RF. Magnetic resonance image of postcraniotomy retained cotton or rayon. Case illustration. J Neurosurg. 1998; 88:928. PMID: 9576268.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reappraising the neurosurgical significance of the pterion location, morphology, and its relationship to optic canal and sphenoid ridge and neurosurgical implications
- Morphological Analysis of the Pterion in Korean
- Textiloma Ten Years after a Lumbar Discectomy: A Case Report
- Comparison between Lateral Supraorbital Approach and Pterional Approach in the Surgical Treatment of Unruptured Intracranial Aneurysms
- Superficial Temporal Artery-Sparing Mini-Pterional Approach for Cerebral Aneurysm Surgery
