Introducer Curving Technique for the Prevention of Tilting of Transfemoral Gunther Tulip Inferior Vena Cava Filter
- Affiliations
-
- 1Department of Radiology, The First Hospital of China Medical University, Shenyang 110001, China. xiaoliangcmu@yahoo.com.cn
- 2Department of Mathematics, College of Basic Medical Science, China Medical University, Shenyang 110001, China.
- KMID: 1383861
- DOI: http://doi.org/10.3348/kjr.2012.13.4.483
Abstract
OBJECTIVE
To determine whether the introducer curving technique is useful in decreasing the degree of tilting of transfemoral Tulip filters.
MATERIALS AND METHODS
The study sample group consisted of 108 patients with deep vein thrombosis who were enrolled and planned to undergo thrombolysis, and who accepted transfemoral Tulip filter insertion procedure. The patients were randomly divided into Group C and Group T. The introducer curving technique was Adopted in Group T. The post-implantation filter tilting angle (ACF) was measured in an anteroposterior projection. The retrieval hook adhering to the vascular wall was measured via tangential cavogram during retrieval.
RESULTS
The overall average ACF was 5.8 +/- 4.14 degrees. In Group C, the average ACF was 7.1 +/- 4.52 degrees. In Group T, the average ACF was 4.4 +/- 3.20 degrees. The groups displayed a statistically significant difference (t = 3.573, p = 0.001) in ACF. Additionally, the difference of ACF between the left and right approaches turned out to be statistically significant (7.1 +/- 4.59 vs. 5.1 +/- 3.82, t = 2.301, p = 0.023). The proportion of severe tilt (ACF > or = 10degrees) in Group T was significantly lower than that in Group C (9.3% vs. 24.1%, chi2 = 4.267, p = 0.039). Between the groups, the difference in the rate of the retrieval hook adhering to the vascular wall was also statistically significant (2.9% vs. 24.2%, chi2 = 5.030, p = 0.025).
CONCLUSION
The introducer curving technique appears to minimize the incidence and extent of transfemoral Tulip filter tilting.
Keyword
MeSH Terms
-
Blood Vessel Prosthesis Implantation/instrumentation/*methods
Chi-Square Distribution
Device Removal
Double-Blind Method
Female
Femoral Vein
Humans
Male
Middle Aged
Prosthesis Design
Pulmonary Embolism/*prevention & control
Statistics, Nonparametric
Thrombolytic Therapy
Treatment Outcome
*Vena Cava Filters
Venous Thrombosis/*complications
Figure
-
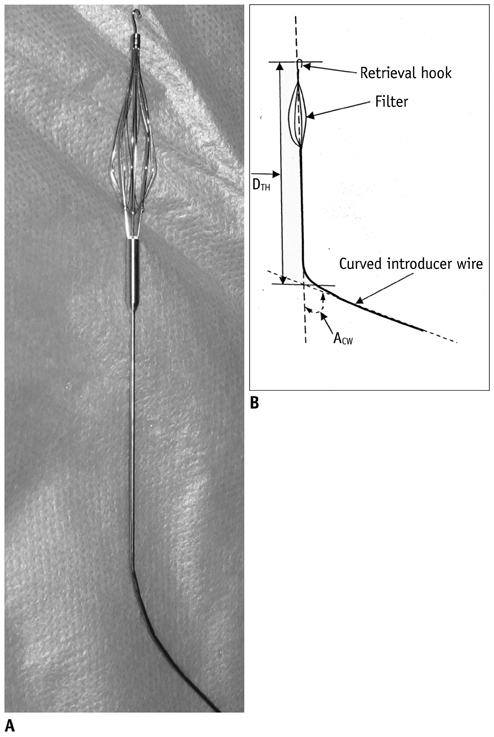
Fig. 1 Photo and line art of curved Günther Tulip filter introducer with filter. A. Photo. B. Line art.

Fig. 2 Procedural step of introducer curving technique. A. Anteroposterior cavogram is performed to document angle (ACI) between inferior vena cava (IVC) and approached iliac vein axis and distance (DRF) between level of lower renal vein confluence and furcation of IVC. B. Metal introducer is curved via introducer curving technique. C. 8.5 Fr sheath is inserted into IVC and filter is placed into sheath and transported into IVC. D. Curved introducer is rotated and orientation of superior segment of introducer is adjusted to parallel with longitude axis of IVC. E. Red hub is loosened and pulled forwards to release filter.

Fig. 3 Concepts and measurement methods of tilting angle (ACF). A. A1 is angle between inferior vena cava axis (A Line) and line (B Line) between spinous processes of L1 and L4 (when vertex of angle locates superior, value of angle is plus). B. A2 is angle between axis of Günther Tulip filter (C Line) and B Line (when vertex of angle locates superior, value of angle is plus). ACF = A1-A2 (when value of ACF is plus, apex of filter tilts to right)

Fig. 4 Relationships between distance (DCH) between caval center and retrieval hook and distance (DTH) between tip of curved angle and apical retrieval hook when introducer curving technique of Günther Tulip filter is adopted. A. When DTH is suitable, DCH is nearly zero. B. When DTH is insufficient, DCH will increase and tilting angle (ACF) will increase. C. When DTH is too high, DCH will increase and ACF will increase.
Reference
-
1. Heit JA. Venous thromboembolism epidemiology: implications for prevention and management. Semin Thromb Hemost. 2002. 28:Suppl 2. 3–13.2. Greenfield LJ, Michna BA. Twelve-year clinical experience with the Greenfield vena caval filter. Surgery. 1988. 104:706–712.3. Pais SO, Tobin KD, Austin CB, Queral L. Percutaneous insertion of the Greenfield inferior vena cava filter: experience with ninety-six patients. J Vasc Surg. 1988. 8:460–464.4. Becker DM, Philbrick JT, Selby JB. Inferior vena cava filters. Indications, safety, effectiveness. Arch Intern Med. 1992. 152:1985–1994.5. Liu WC, Do YS, Choo SW, Kim DI, Kim YW, Kim DK, et al. The mid-term efficacy and safety of a permanent nitinol IVC filter (TrapEase). Korean J Radiol. 2005. 6:110–116.6. Kinney TB. Update on inferior vena cava filters. J Vasc Interv Radiol. 2003. 14:425–440.7. Berczi V, Bottomley JR, Thomas SM, Taneja S, Gaines PA, Cleveland TJ. Long-term retrievability of IVC filters: should we abandon permanent devices? Cardiovasc Intervent Radiol. 2007. 30:820–827.8. PREPIC Study Group. Eight-year follow-up of patients with permanent vena cava filters in the prevention of pulmonary embolism: the PREPIC (Prevention du Risque d'Embolie Pulmonaire par Interruption Cave) randomized study. Circulation. 2005. 112:416–422.9. Looby S, Given MF, Geoghegan T, McErlean A, Lee MJ. Gunther Tulip retrievable inferior vena caval filters: indications, efficacy, retrieval, and complications. Cardiovasc Intervent Radiol. 2007. 30:59–65.10. Wicky S, Doenz F, Meuwly JY, Portier F, Schnyder P, Denys A. Clinical experience with retrievable Günther Tulip vena cava filters. J Endovasc Ther. 2003. 10:994–1000.11. Rosenthal D, Wellons ED, Hancock SM, Burkett AB. Retrievability of the Günther Tulip vena cava filter after dwell times longer than 180 days in patients with multiple trauma. J Endovasc Ther. 2007. 14:406–410.12. Hoppe H, Nutting CW, Smouse HR, Vesely TM, Pohl C, Bettmann MA, et al. Günther Tulip filter retrievability multicenter study including CT follow-up: final report. J Vasc Interv Radiol. 2006. 17:1017–1023.13. Lopera JE, Araki JU, Kirsch D, Qian Z, Brazzini A, Gonzalez A, et al. A modified technique to minimize filter tilting during deployment of the Günther Tulip filter: in vitro study. J Vasc Interv Radiol. 2005. 16:1539–1544.14. Van Ha TG, Vinokur O, Lorenz J, Regalado S, Zangan S, Piano G, et al. Techniques used for difficult retrievals of the Günther Tulip inferior vena cava filter: experience in 32 patients. J Vasc Interv Radiol. 2009. 20:92–99.15. Joels CS, Sing RF, Heniford BT. Complications of inferior vena cava filters. Am Surg. 2003. 69:654–659.16. Kinney TB, Rose SC. Regarding "Limb asymmetry in titanium Greenfield filters: clinically significant?". J Vasc Surg. 1998. 27:1193–1194.17. Neuerburg J, Günther RW, Rassmussen E, Vorwerk D, Tonn K, Handt S, et al. New retrievable percutaneous vena cava filter: experimental in vitro and in vivo evaluation. Cardiovasc Intervent Radiol. 1993. 16:224–229.18. Terhaar OA, Lyon SM, Given MF, Foster AE, Mc Grath F, Lee MJ. Extended interval for retrieval of Günther Tulip filters. J Vasc Interv Radiol. 2004. 15:1257–1262.19. Sag AA, Stavas JM, Burke CT, Dixon RG, Marquess JS, Mauro MA. Analysis of tilt of the Günther Tulip filter. J Vasc Interv Radiol. 2008. 19:669–676.20. Seo TS, Cha IH, Park CM, Kim KA, Lee CH, Choi JW, et al. Detection and correction of anterior or posterior tilting of the Günther-Tulip filter in the inferior vena cava and correction by repositioning: a phantom study and preliminary clinical experiences. J Vasc Interv Radiol. 2007. 18:427–436.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Spontaneous Tilting after Placement of the Gunther-Tulip Inferior Vena Caval Filter: A Case Report
- Fracture and Embolization of a Celect Inferior Vena Cava Filter Strut to the Liver: A Case Report
- Placement and Retrieval of a Gunther Tulip Filter in Patients with a Free Floating Thrombus in Inferior Vena Cava
- Surgical Removal of the Inferior Vena Cava Filter Using Minimal Cavotomy: A Case Report
- Suprarenal Filter Placement in the Inferior Vena Cava to Prevent Tumor Emboli During Radical Nephrectomy in Renal Cell Carcinoma Invading the Inferior Vena Cava
