Korean J Urol.
2008 Nov;49(11):1024-1028. 10.4111/kju.2008.49.11.1024.
Efficacy of the Modified STING Procedure for the Treatment of High Grade Vesicoureteral Reflux
- Affiliations
-
- 1Department of Urology, College of Medicine, Korea University, Seoul, Korea. dgmoon@korea.ac.kr
- KMID: 1328176
- DOI: http://doi.org/10.4111/kju.2008.49.11.1024
Abstract
-
PURPOSE: The modified subureteral transurethral injection(STING) has been reported to increase the success of endoscopic treatment of high grade vesicoureteral reflux(VUR). This study was performed to assess the efficacy of the modified STING procedure compared to conventional STING in the setting of high grade VUR.
MATERIALS AND METHODS
We retrospectively reviewed the medical records of 40 consecutive children(46 ureters) with a median age of 5.32 years (range 1 to 10 years) who underwent endoscopic treatment of grade IV to grade V VUR between February 2004 and December 2006. The modified STING was performed by applying a direct pressure stream of irrigation fluid into the ureter in order to define the injection site within the ureteral submucosa. The needle was then placed in the ureteral tunnel, and a dextranomer/hyaluronic acid copolymer(Dx/HA) was injected into the submucosal intraureteral space, tracking along the entire length of the detrusor tunnel. Modified STING was performed in 27 ureters(grade IV: 13, grade V: 14), and conventional STING was performed in 19 ureters (grade IV: 12, grade V: 7). Follow-up voiding cystourethrography(VCUG) was performed 3 months later.
RESULTS
Complete resolution occurred in 82%(22/27 ureters) of the patients undergoing modified STING, including 92%(12/13) of grade IV patients and 71%(10/14) of grade V patients. Three ureters required a second injection to correct VUR. Conventional STING had a success rate of 63%(12/19), [75%(9/12) in grade IV and 43%(3/7) in grade V]. The mean injected volume for the modified STING was 1.23+/-0.3ml, while that for the conventional STING was 0.95+/-0.2ml(p=0.03).
Conclusions
The modified STING was markedly more successful in the treatment of high grade VUR and carried no significant adverse effects.
MeSH Terms
Figure
-

Fig. 1 Follow-up voiding cystourethrography showing recurrence after modified subureteral transurethral injection (STING). A filling defect (arrow) highlights injected material in the submucosal intraureteral space after modified STING.
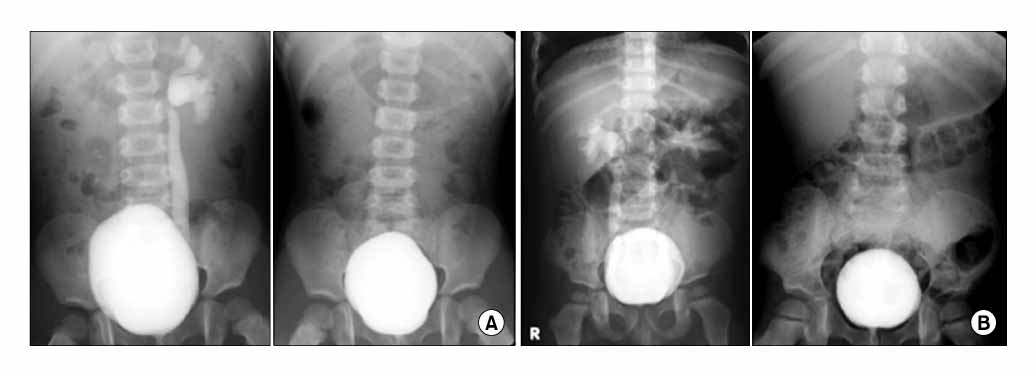
Fig. 2 (A) Voiding cystourethrography showing grade IV vesicoureteral reflux. Three months later, a follow-up voiding cystourethrography shows complete resolution after modified subureteral transurethral injection (STING). (B) Voiding cystourethrography showing bilateral vesicoureteral reflux (Rt: grade IV, Lt: grade III). Three months later, a follow-up voiding cystourethrography shows complete resolution after modified STING.
Reference
-
1. Capozza N, Lais A, Matarazzo E, Nappo S, Patricolo M, Caione P. Treatment of vesico-ureteric reflux: a new algorithm based on parental preference. BJU Int. 2003. 92:285–288.2. Capozza N, Lais A, Nappo S, Caione P. The role of endoscopic treatment of vesicoureteral reflux: a 17-year experience. J Urol. 2004. 172:1626–1628.3. Kim HC, Shim KS, Moon DG. The early experience and technical aspects of endoscopic subureteral polydimethylsiloxane injection for vesicoureteral reflux. Korean J Urol. 2006. 47:154–159.4. Kirsch AJ, Perez-Brayfield M, Smith EA, Scherz HC. The modified sting procedure to correct vesicoureteral reflux: improved results with submucosal implantation within the intramural ureter. J Urol. 2004. 171:2413–2416.5. Elder JS, Peters CA, Arant BS Jr, Ewalt DH, Hawtrey CE, Hurwitz RS, et al. Pediatric vesicoureteral reflux guidelines panel summary report on the management of primary vesicoureteral reflux in children. J Urol. 1997. 157:1846–1851.6. Lebowitz RL, Olbing H, Parkkulainen KV, Smellie JM, Tamminen-Mobius TE. International system of radiographic grading of vesicoureteric reflux. International reflux study in children. Pediatr Radiol. 1985. 15:105–109.7. Koyle MA, Caldamone AA. Part 4: considerations regarding the medical management of VUR: What have we really learned? Curr Med Res Opin. 2007. 23:Suppl 4. S21–S25.8. Schwab CW Jr, Wu HY, Selman H, Smith GH, Snyder HM 3rd, Canning DA. Spontaneous resolution of vesicoureteral reflux: a 15-year perspective. J Urol. 2002. 168:2594–2599.9. Capozza N, Caione P. Dextranomer/hyaluronic acid copolymer implantation for vesico-ureteral reflux: a randomized comparison with antibiotic prophylaxis. J Pediatr. 2002. 140:230–234.10. Matouschek E. Treatment of vesicorenal reflux by transurethral teflon-injection (author's transl). Urologe A. 1981. 20:263–264.11. O'Donnell B, Puri P. Treatment of vesicoureteric reflux by endoscopic injection of Teflon. Br Med J. 1984. 289:7–9.12. Puri P, O'Donnell B. Correction of experimentally produced vesicoureteric reflux in the piglet by intravesical injection of Teflon. Br Med J. 1984. 289:5–7.13. Puri P, Pirker M, Mohanan N, Dawrant M, Dass L, Colhoun E. Subureteral dextranomer/hyaluronic acid injection as first line treatment in the management of high grade vesicoureteral reflux. J Urol. 2006. 176:1856–1859.14. Diamond DA, Caldamone AA, Bauer SB, Retik AB. Mechanisms of failure of endoscopic treatment of vesicoureteral reflux based on endoscopic anatomy. J Urol. 2003. 170:1556–1558.15. Higham-Kessler J, Reinert SE, Snodgrass WT, Hensle TW, Koyle MA, Hurwitz RS, et al. A review of failures of endoscopic treatment of vesicoureteral reflux with dextranomer microspheres. J Urol. 2007. 177:710–714.16. Dawrant MJ, Mohanan N, Puri P. Endoscopic treatment for high grade vesicoureteral reflux in infants. J Urol. 2006. 176:1847–1850.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Does the Modified STING Method Increase the Success Rate in the Management of Moderate or High-Grade Reflux?
- Efficacy of Hydrodistention Implantation Technique in Treating High-Grade Vesicoureteral Reflux
- Reflux Nephropathy in Children
- Unusual Case of Vesicoureteral Reflux and Chronic Kidney Disease in a 10-Year-old Boy with Asymptomatic Bacteriuria
- Vesicoureteral Reflux in Patients with Double-J Stent
