Nodular Fasciitis with Cortical Erosion of the Hand
- Affiliations
-
- 1Department of Orthopaedic Surgery, Gyeongsang National University Hosptial, Gyeongsang National University School of Medicine, Jinju, Korea. hbinpark@gnu.ac.kr
- 2Department of Pathology, Gyeongsang National University Hosptial, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Department of Radiology, Gyeongsang National University Hosptial, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 1245405
- DOI: http://doi.org/10.4055/cios.2012.4.1.98
Abstract
- Nodular fasciitis is a benign, reactive myofibroblastic tumor that is often mistaken for a sarcoma because of its histological appearance and rapid growth. Involvement of a finger is extremely rare. We report a case of nodular fasciitis of the thumb, accompanied by bone erosion. Magnetic resonance findings suggested the possibility of a malignancy, which could have led to misdiagnosis as a malignant soft tissue sarcoma. Instead, the lesion was treated by excisional biopsy, which confirmed nodular fasciitis. There has been no evidence of local recurrence at recent follow-up, 1 year after surgery. This case illustrates that, to avoid unnecessarily aggressive surgery, nodular fasciitis must be included in the differential diagnosis for any finger lesion that resembles a sarcoma, even if bone erosion is present.
Keyword
MeSH Terms
Figure
-

Fig. 1 A photograph showing the soft tissue mass, approximately 2 cm in diameter and located on the radial side of the proximal phalanx of the right thumb.

Fig. 2 (A) Anteroposterior and (B) lateral plain radiographs reveal the bone erosion of the radial side proximal phalanx close to the soft tissue mass.
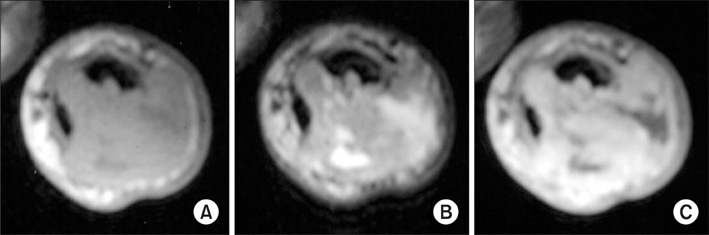
Fig. 3 Magnetic resonance images reveal that the well-circumscribed soft tissue mass, measuring 1.4 × 2.3 × 1.5 cm, has invaded the cortex and bone marrow of the mid-shaft of the proximal phalanx. The mass shows (A) iso-signal intensity on T1-weighted images, (B) heterogeneous, slightly high, signal intensity on T2-weighted images, and (C) strong enhancement on enhanced T1-weighted images.
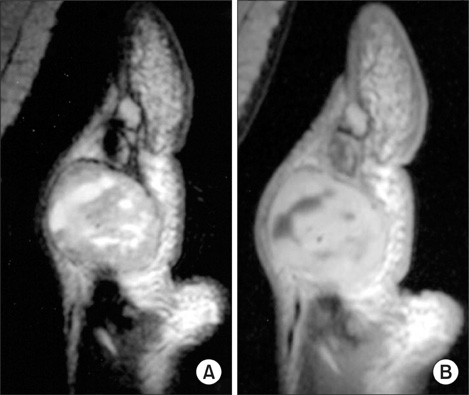
Fig. 4 The mass shows some areas with (A) high signal intensity on T2-weighted images, and (B) no enhancement on enhanced T1-weighted images. This suggests that the mass might include necrotic or hemorrhagic components.

Fig. 5 A high-power view shows plump, randomly oriented spindle cells surrounded by myxoid stroma. Although cellularity of the lesion was high, hyperchromatism and variation in the size and shape of the nuclei were mild. Mitotic activity ranged from 5 to 10 mitotic figures per 10 high-power fields, with no atypical forms identified (H&E, × 200).
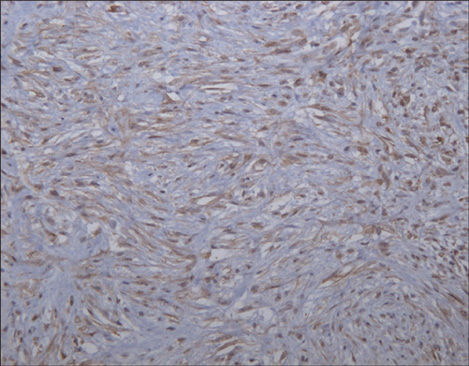
Fig. 6 In immunohistochemical staining, tumor cells were positive for alpha-smooth muscle actin (alpha-smooth muscle actin, × 200).
Reference
-
1. Bernstein KE, Lattes R. Nodular (pseudosarcomatous) fasciitis, a nonrecurrent lesion: clinicopathologic study of 134 cases. Cancer. 1982. 49(8):1668–1678.
Article2. Katz MA, Beredjiklian PK, Wirganowicz PZ. Nodular fasciitis of the hand: a case report. Clin Orthop Relat Res. 2001. (382):108–111.3. Rankin G, Kuschner SH, Gellman H. Nodular fasciitis: a rapidly growing tumor of the hand. J Hand Surg Am. 1991. 16(5):791–795.
Article4. Wang XL, De Schepper AM, Vanhoenacker F, et al. Nodular fasciitis: correlation of MRI findings and histopathology. Skeletal Radiol. 2002. 31(3):155–161.
Article5. Konwaler BE, Keasbey L, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol. 1955. 25(3):241–252.
Article6. Shimizu S, Hashimoto H, Enjoji M. Nodular fasciitis: an analysis of 250 patients. Pathology. 1984. 16(2):161–166.
Article7. Kransdorf MJ, Murphey MD. Imaging of soft tissue tumors. 1997. Philadelphia, PA: Saunders;143–186.8. Singh R, Sharma AK. Nodular fasciitis of the thumb: a case report. Hand Surg. 2004. 9(1):117–120.
Article9. Le Corroller T, Kovacs TJ, Champsaur P. Nodular fasciitis with cortical involvement. Joint Bone Spine. 2009. 76(1):101–103.
Article10. Park C, Park J, Lee KY. Parosteal (nodular) fasciitis of the hand. Clin Radiol. 2004. 59(4):376–378.
Article
