Free Fat Graft for Congenital Hand Differences
- Affiliations
-
- 1Sapporo Hand Surgery and Congenital Hand Differences Center, Orthopaedic Hokushin-Higashi Hospital, Sapporo, Japan. hand@ogino1.com
- 2Department of Orthopaedic Surgery, Yamagata University School of Medicine, Yamagata, Japan.
- 3Department of Orthopaedic Surgery, Sapporo Medical University School of Medicine, Sapporo, Japan.
- KMID: 1245398
- DOI: http://doi.org/10.4055/cios.2012.4.1.45
Abstract
- BACKGROUND
Free fat graft has been used for the treatment of congenital hand differences. However, there have been a few reports about the outcome of that treatment. In this study, the outcome of free fat grafts for congenital hand and foot differences was investigated.
METHODS
Fourteen bones with longitudinal epiphyseal bracket, 3 wrists with Madelung deformity, and 5 cases of osseous syndactyly were treated with free fat graft with osteotomy, physiolysis, or separation of osseous syndactyly. Of the fourteen bones with longitudinal epiphyseal bracket, 9 were treated with open wedge osteotomy with free fat graft and 5 with physiolysis and free fat graft. The Madelung deformity was treated with physiolysis with free fat graft. For osseous syndactyly, syndactyly release with free fat graft was performed five times on four hands.
RESULTS
In the fourteen cases with longitudinal epiphyseal bracket, lateral deviation improved in all except two cases after surgery. The average lateral deviation angle changed from 32.5 degrees before surgery to 15.2 degrees after surgery. The average improvement of the lateral deviation angle was 12.2 degrees in the osteotomy group and 20.6 degrees in the physiolysis group. The mean ratio of improvement of the lateral deviation angle to the lateral deviation angle before surgery was 39.4% in the osteotomy group and 51.2% in the physiolysis group. The Madelung deformity improved after surgery in two cases but there was no improvement in one case. For these conditions, the results were not good enough when surgery was done after age 13 or at age four for severely hypoplastic brachymesophalangy. Of the 5 cases of osseous syndactyly, reunion of the separated bones occurred in one case. The grafted free fat should be deep enough to cover the osteotomy site of the bones to prevent reunion of the separated bones.
CONCLUSIONS
Physiolysis and free fat graft performed during the growth period can correct the deviation due to longitudinal epiphyseal bracket and Madelung deformity. Free fat graft is also useful to prevent reunion of the bones after separation of osseous syndcatyly, if the grafted fat is securely filled into the space between the separated bones.
Keyword
MeSH Terms
Figure
-
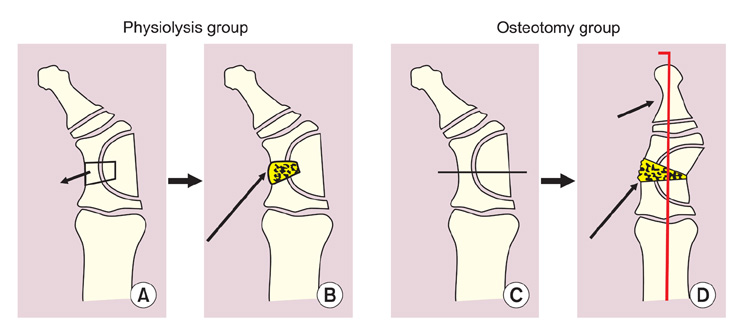
Fig. 1 Procedures for the longitudinal epiphyseal bracket. Two kind of procedures have been performed for the longitudinal epiphyseal bracket. (A, B) In the physiolysis group, the midzone of the longitudinal epiphyseal bracket was excised as shown with the small arrow and replaced with free fat graft as shown with the long arrow. (C, D) In the osteotomy group, an open wedge osteotomy was performed at the midzone of the phalanges as shown with the transverse line and the deviation was corrected as shown with the small arrow. Then the gap was filled with free fat graft as shown with the long arrow. Reprinted with permission from Japanese Society for Surgery of the Hand.9)

Fig. 2 Postoperative evaluation of the physiolysis for the longitudinal epiphyseal bracket and the Madelung deformity. (A) Lateral deviation angle (LDA): LDA is defined as the angle between the longitudinal axis of the metacarpal bone (a) and that of the distal and proximal phalanges (b) of the affected digit or toe. (B) Inclination of the distal radius: The inclination of the distal radius is defined as the angle between the perpendicular line (c) of the longitudinal axis of the radius and the line of the distal articular surface of the radius (d) by using an AP view of the roentgenogram. (C) Palmar shift of the hand: Palmar shift of the hand is defined as the ratio of the shortest distance (f) between the scaphoid tubercle and the extension line of the palmar cortex of the radial shaft to the width (e) of the radial shaft by using a lateral view of the roentgenogram. Reprinted with permission from Japanese Society for Surgery of the Hand.9)

Fig. 3 Physiolysis with free fat graft for the Madelung deformity according to Vickers procedure. (A) Through the palmar approach, the radiolunate ligament was removed and the bone block connecting the epiphsis across the physis to the metaphysis of the distal radius was removed an shown with the oblique long arrow. (B) A dotted area, where the bone block was removed, was packed with free fat graft and was fixed there by suturing the surrounding tissue such as periosteum or the holes of the cortex of the radius. Holes of the bone were made with a Kirshner wire. Reprinted with permission from Japanese Society for Surgery of the Hand.9)
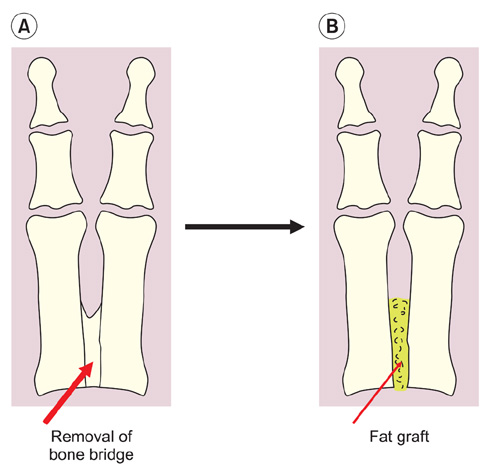
Fig. 4 Free fat graft after separation of the osseous syndactyly. Excision of the bone bridge (A) and replacement with free fat graft (B) was performed.

Fig. 5 Case #7, left hand: clinodactyly of the little finger due to the longitudinal epiphseal bracket of the middle phalanx. Excision of the midzone of the longitudinal epiphyseal bracket combined with free fat graft was performed on the middle phalanx at the age of 6. The lateral deviation angle was 44 degrees before surgery.

Fig. 6 Case #7, right hand at the age of 15. The lateral deviation angle was improved to 13 degrees 7 years after surgery. In this case, 31 degrees of spontaneous correction has been achieved.
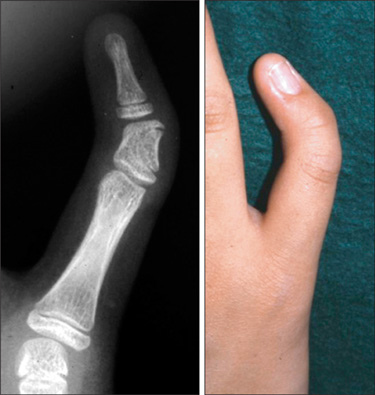
Fig. 7 Case #7, right hand of a 13-year-old girl. Clinodactyly of the little finger due to the longitudinal epiphyseal bracket. The patient seemed too old to be treated with physiolysis only. The open wedge osteotomy of the middle phalanx was performed and the space was packed with free fat graft. The lateral deviation angle was 40 degrees before surgery.

Fig. 8 Case #7, left hand at the age of 13. The lateral deviation angle was corrected 10 degrees 2 years after surgery. Thirty degrees of deviation still remained, but the improvement of the shape of middle phalanx had been obtained.
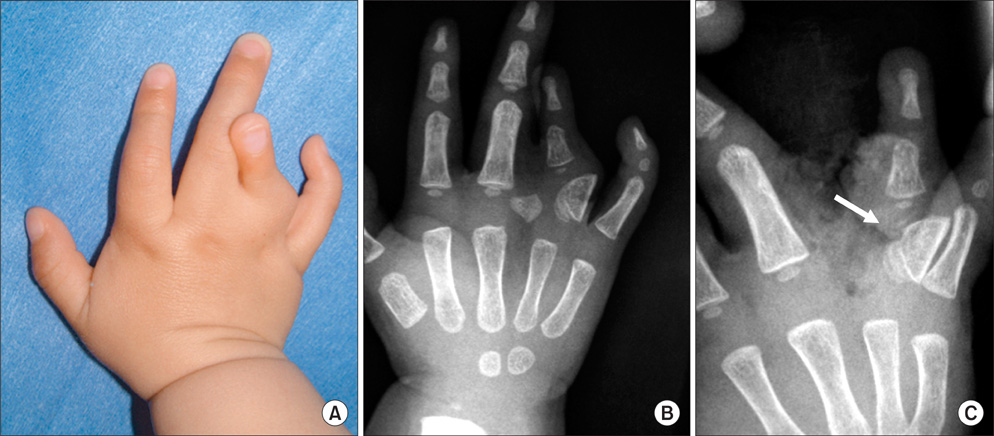
Fig. 9 Case #8, right hand of a 2-year-old boy. Synpolydactyly with a cross bone and the longitudinal epiphyseal bracket of the ring finger. (A) There was cutaneous syndactyly and overlapping of the middle and ring fingers due to deviation of the ring finger. (B) Roentgenogram revealed the longitudinal epiphyseal bracket of the proximal phalanx of the ring finger and a cross bone between the middle and ring fingers. (C) The roentgenogram after removal of the cross bone and physiolysis followed with free fat graft.

Fig. 10 Case #8, the appearance and roentgenogram 8 years after surgery. (A) The ring finger was short, but the deviation at follow-up was improved compared to before surgery. (B) The shape of proximal phalanx changed from a D shape before surgery to trapezoidal shape at follow-up.
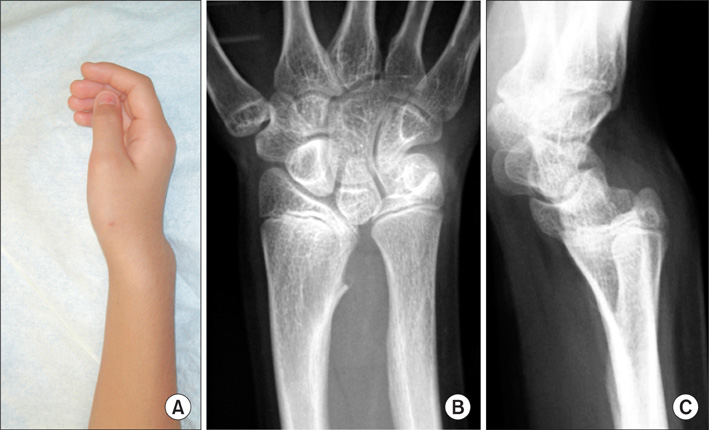
Fig. 11 Case #11, the Madelung deformity treated with physiolysis and free fat graft. (A) The appearance of the wrist deformity was typical of the Madelung deformity. (B) AP view roentgenogram of the wrist revealed a bone bridge formed prematurely across the physis of the ulnar side of the distal radius. The ulnar head was overlapped with the lunate and triquetrum. (C) Lateral view roentgenogram of the wrist revealed dorsal subluxation of the ulnar head and a palmar shift of the carpal bones.

Fig. 12 Case #11, postoperative roentgenograms. (A) Two months after surgery. (B, C) Five months after surgery. No bony bride formation was observed across the physis of the distal radius.

Fig. 13 Case #11, the appearance and roentgenograms 12 months after surgery. (A) The appearance of the wrist deformity was improved. (B) The prominence of the ulnar head was reduced. (C) Ulnar inclination was reduced and the overlapping between the ulnar head and carpal bones disappeared. (D) Dorsal subluxation of the ulnar head seemed to be reduced. The palmar shift of the carpal bones was improved.
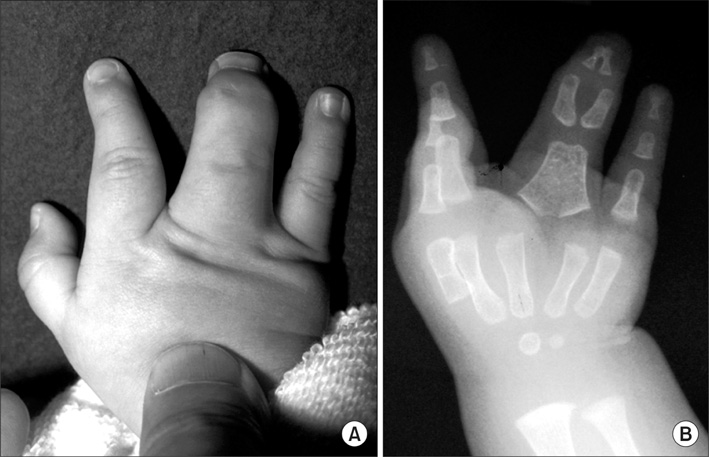
Fig. 14 Case #14, a one-year-old boy with osseous syndactyly of the right hand. (A) The appearance: there is a common nail of the middle and ring fingers. (B) Roentgenogram: the distal ends of the distal phalanges fused osseously. The proximal phalanges of these fingers fused completely.
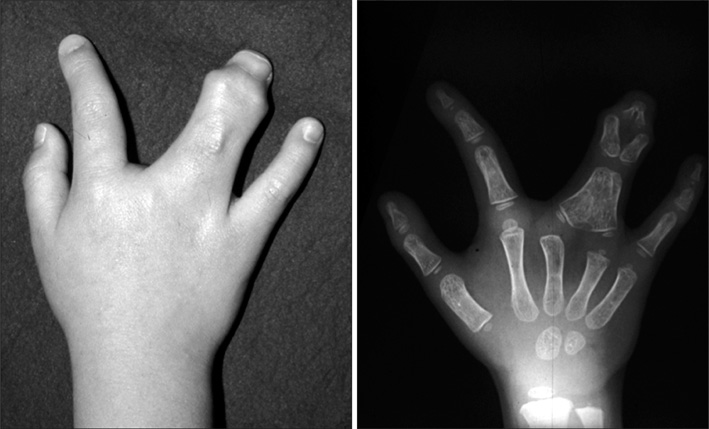
Fig. 15 Case #14, the appearance and roentgenogram at the age of three. The width of the distal interphalangeal joints of the syndactylous fingers became wider, because the direction of the growth of the distal phalanges were changed due to the osseous union of the tip of the distal phalanges of the middle and ring fingers.

Fig. 16 Case #14, roentgenogram at the age of six. (A) The united distal phalanges were separated and the space between these phalanges was filled with free fat graft at the age of three, but there was no recurrence of the bone union. (B) This was a roentgenogram 7 weeks after the syndactyly release of the middle and ring fingers. The united proximal phalanges were separated and the space between these phalanges was filled with free fat graft. The distal interphalangeal joint of the middle finger was unstable and it was fixed with a Kirschner wire for 8 weeks.

Fig. 17 Case #14, roentgenograms at the age of 13. (A) The reunion of the proximal part of the proximal phalanx occurred at the age of 8 (two and one-half years after the syndactyly release), but it was not treated surgically. The patient sustained a distal phalangeal fracture at the age of 13. (B) The fracture was fixed with modified interosseous wiring and the osseous union of the proximal phalanges of the middle and ring fingers was removed and free fat was grafted into the separated phalanges. (C) One year after the last surgery, there was no bony union of the phalanges.
Reference
-
1. Langenskiold A. The possibilities of eliminating premature partial closure of an epiphyseal plate caused by trauma or disease. Acta Orthop Scand. 1967. 38(1-4):267–279.
Article2. Langenskiold A. An operation for partial closure of an epiphysial plate in children, and its experimental basis. J Bone Joint Surg Br. 1975. 57(3):325–330.3. Light TR, Ogden JA. The longitudinal epiphyseal bracket: implications for surgical correction. J Pediatr Orthop. 1981. 1(3):299–305.
Article4. Vickers D. Clinodactyly of the little finger: a simple operative technique for reversal of the growth abnormality. J Hand Surg Br. 1987. 12(3):335–342.
Article5. Vickers D, Nielsen G. Madelung deformity: surgical prophylaxis (physiolysis) during the late growth period by resection of the dyschondrosteosis lesion. J Hand Surg Br. 1992. 17(4):401–407.
Article6. Zhang G, Kato H, Yamazaki H. Physiolysis for correction of the delta phalanx in clinodactyly of the bilateral little fingers. Hand Surg. 2005. 10(2-3):297–302.
Article7. Bednar MS, Bindra RR, Light TR. Epiphyseal bar resection and fat interposition for clinodactyly. J Hand Surg Am. 2010. 35(5):834–837.
Article8. Kato H, Ogino T, Minami A, Sugimoto Y, Nakatsuchi Y. Delta pahalnax: roetntgenographic findings and surgical treatment. J Jpn Soc Surg Hand. 1990. 6(6):1031–1041.9. Ishigaki D, Ogino T, Takahara M, Kikuchi N, Watanabe T. Pysiolysis and free fat graft for congenital growth plate disorders. J Jpn Soc Surg Hand. 2007. 24(3):306–311.10. Jonew GB. Delta phalanx. J Bone Joint Surg Br. 1964. 46(2):226–228.11. Carstam N, Theander G. Surgical treatment of clinodactyly caused by longitudinally bracketed diaphysis ("delta phalanx"). Scand J Plast Reconstr Surg. 1975. 9(3):199–202.
Article12. Swanson AB, Swanson GD, Tada K. A classification for congenital limb malformation. J Hand Surg Am. 1983. 8(5 Pt 2):693–702.
Article13. Jaeger M, Refior HJ. The congenital triangular deformity of the tubular bones of hand and foot. Clin Orthop Relat Res. 1971. 81:139–150.
Article14. Congenital Committee of the Japanese Society for Surgery of the Hand. A manual for classification of congenital hand deformities. J Jpn Soc Surg Hand. 2000. 17(3):353–365.15. Smith RJ. Osteotomy for "delta-phalanx" deformity. Clin Orthop Relat Res. 1977. (123):91–94.
Article16. White GM, Weiland AJ. Madelung's deformity: treatment by osteotomy of the radius and Lauenstein procedure. J Hand Surg Am. 1987. 12(2):202–204.
Article17. Sakuma T, Ogino T, Minami A, Fukuda K, Muramatsu I. Clinical features of Madelung's deformity and functional results after surgery. J Jpn Soc Surg Hand. 1987. 4(2):586–592.18. Watson HK, Pitts EC, Herber S. Madelung's deformity: a surgical technique. J Hand Surg Br. 1993. 18(5):601–605.19. Langenskiold A, Kiviluoto O. Prevention of epidural scar formation after operations on the lumbar spine by means of free fat transplants: a preliminary report. Clin Orthop Relat Res. 1976. (115):92–95.20. Kanaya F, Ibaraki K. Mobilization of a congenital proximal radioulnar synostosis with use of a free vascularized fascio-fat graft. J Bone Joint Surg Am. 1998. 80(8):1186–1192.
Article21. Ueba Y, Nishijima N, Takada H. Congenital synostosis of the fourth and fifth metacarpal. Seikei Geka. 1983. 34(12):1810–1812.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Congenital hand differences: a comprehensive literature review
- Congenital Pseudarthrosisof the Tibia: Treated with Free Vascularized Fibular Graft
- Management of the Posttraumatic Neuralgia of the Peripheral Nerve by External Neurolysis
- Cauda Equina Syndrome after Laminectomy of Lumbar Spine with Application of Autogenous Free Fat Graft: A Case Report
- Correction of the Tear Trough Using Orbital Fat Graft from the Lower Lid
