Reevaluation of the Pavlov Ratio in Patients with Cervical Myelopathy
- Affiliations
-
- 1Department of Orthopedic Surgery, Kyung Hee University College of Medicine, Korea. sks@khmc.or.kr
- 2Seoul Medical Center, Seoul, Korea.
- KMID: 1127908
- DOI: http://doi.org/10.4055/cios.2009.1.1.6
Abstract
-
BACKGROUND: This study was designed to reevaluate the effectiveness of the Pavlov ratio in patients with cervical myelopathy.
METHODS
We studied 107 patients who underwent open door laminoplasty for the treatment of cervical myelopathy between the C3 to C7 levels. We determined the Pavlov ratio on preoperative and postoperative cervical spine lateral radiographs, the vertebral body-to-canal ratio on sagittal reconstruction CT scans, and the vertebral body-to-cerebrospinal fluid (CSF) column ratio on T2-weighted sagittal MR images from C3 to C6. The severity of myelopathy was determined using the JOA score on both preoperative and postoperative images. The recovery rate was also calculated. The Pavlov ratio in plain radiographs from patients with myelopathy was compared with the ratio of the vertebral body to the spinal canal on CT and MRI.
RESULTS
The average Pavlov ratio between C3 and C6 ranged from 0.71 to 0.76. On CT scan, the average vertebral body-to-canal ratio between C3 and C6 ranged from 0.62 to 0.66. On MRI, the vertebral body-to-CSF column ratio between C3 and C6 ranged between 0.53 and 0.57. A positive correlation was noted between the Pavlov ratio and the vertebral body-to-canal ratio on sagittal-reconstruction CT (correlation coefficient = 0.497-0.627, p = 0.000) and between the Pavlov ratio and the vertebral body-to-CSF column ratio on MRI (correlation coefficient = 0.511-0.649, p = 0.000).
CONCLUSIONS
We demonstrated a good correlation between the Pavlov ratio and both the vertebral body-to-canal ratio on CT and the vertebral body-to-CSF column ratio on MRI. Therefore, the Pavlov ratio can be relied upon to predict narrowing of the cervical spinal canal in the sagittal plane.
Keyword
MeSH Terms
-
Adult
Aged
Aged, 80 and over
Cerebrospinal Fluid
Cervical Vertebrae/*pathology/*radiography/surgery
Female
Humans
*Magnetic Resonance Imaging
Male
Middle Aged
Observer Variation
Predictive Value of Tests
Reference Values
Retrospective Studies
Spinal Canal/radiography
Spinal Cord Diseases/*pathology/*radiography
*Tomography, X-Ray Computed
Figure
-

Fig. 1 The sagittal diameter of the spinal canal (a) is measured from the posterior surface of the vertebral body to the nearest point of the corresponding spinal laminar line. The sagittal diameter of the vertebral body (b) is measured at the midpoint between the anterior surface and the posterior surface. The spinal canal/vertebral body ratio is determined using the formula a/b.

Fig. 2 On the CT image, the diameters of the spinal canal (a) and vertebral body (b) are measured at the midvertebral level on sagittal-reconstructed CT images. The spinal canal/vertebral body ratio is determined using the formula a/b.
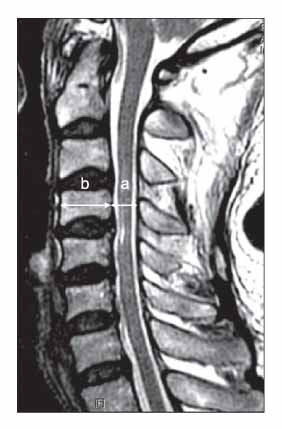
Fig. 3 On the MR image, the sagittal diameters of the CSF column (a) and vertebral body (b) are measured at the midvertebral level on T2 sagittal images. The CSF column/vertebral body ratio is determined using the formula a/b.
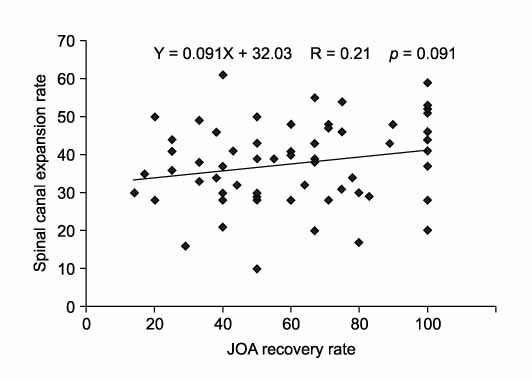
Fig. 4 The correlation between JOA recovery rate and spinal canal expansion rate. The spinal canal expansion rate showed no significant correlation (r = 0.21, p > 0.05) with JOA recovery rate.
Reference
-
1. Herzog RJ, Wiens JJ, Dillingham MF, Sontag MJ. Normal cervical spine morphometry and cervical spinal stenosis in asymptomatic professional football players. Plain film radiography, multiplanar computed tomography, and magnetic resonance imaging. Spine. 1991. 16(6 Suppl):S178–S186.2. Payne EE, Spillane JD. The cervical spine; an anatomicopathological study of 70 specimens (using a special technique) with particular reference to the problem of cervical spondylosis. Brain. 1957. 80(4):571–596.
Article3. Edwards WC, LaRocca H. The developmental segmental sagittal diameter of the cervical spinal canal in patients with cervical spondylosis. Spine. 1983. 8(1):20–27.
Article4. Hayashi H, Okada K, Hamada M, Tada K, Ueno R. Etiologic factors of myelopathy. A radiographic evaluation of the aging changes in the cervical spine. Clin Orthop Relat Res. 1987. (214):200–209.5. Murone I. The importance of the sagittal diameters of the cervical spinal canal in relation to spondylosis and myelopathy. J Bone Joint Surg Br. 1974. 56(1):30–36.6. Chrispin AR, Lees F. The spinal canal in cervical spondylosis. J Neurol Neurosurg Psychiatry. 1963. 26:166–170.
Article7. Ehni G. Cervical arthrosis: disease of cervical motion segments (spondylosis, disk rupture, radiculopathy and myelopathy). 1984. Chicago: Yearbook Medical;26–43. 84–90.8. Pavlov H, Torg JS, Robie B, Jahre C. Cervical spinal stenosis: determination with vertebral body ratio method. Radiology. 1987. 164(3):771–775.
Article9. Yue WM, Tan SB, Tan MH, Koh DC, Tan CT. The Torg-Pavlov ratio in cervical spondylotic myelopathy: a comparative study between patients with cervical spondylotic myelopathy and a nonspondylotic, nonmyelopathic population. Spine. 2001. 26(16):1760–1764.
Article10. Blackley HR, Plank LD, Robertson PA. Determining the sagittal dimensions of the canal of the cervical spine. The reliability of ratios of anatomical measurements. J Bone Joint Surg Br. 1999. 81(1):110–112.11. Moskovich R, Shott S, Zhang ZH. Does the cervical canal to body ratio predict spinal stenosis? Bull Hosp Jt Dis. 1996. 55(2):61–71.12. Hukuda S, Xiang LF, Imai S, Katsuura A, Imanaka T. Large vertebral body, in addition to narrow spinal canal, are risk factors for cervical myelopathy. J Spinal Disord. 1996. 9(3):177–186.
Article13. Chen IH, Liao KK, Shen WY. Measurement of cervical canal sagittal diameter in Chinese males with cervical spondylotic myelopathy. Zhonghua Yi Xue Za Zhi (Taipei). 1994. 54(2):105–110.14. Bohlman HH, Emery SE. The pathophysiology of cervical spondylosis and myelopathy. Spine. 1988. 13(7):843–846.
Article15. Hukuda S, Mochizuki T, Ogata M, Shichikawa K, Shimo-mura Y. Operations for cervical spondylotic myelopathy A comparison of the results of anterior and posterior procedures. J Bone Joint Surg Br. 1985. 67(4):609–615.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pavlov’s Ratio of the Cervical Spine in a Korean Population: A Comparative Study by Age in Patients with Minor Trauma without Neurologic Symptoms
- Anterior Cervical Decompression and Fusion for the Treatment of Cervical Spondylotic Myelopathy
- Evaluation of Factors on Clinical Results Following Expansive Laminoplasty for Cervical Myelopathy
- Pavlov's Ratio of Cervical Spine of Normal Koreans : Determining Spinal Stenosis on Routine Lateral Roentgenograms
- The Relationship between Spinal Stenosis and Neurological Outcome in Traumatic Cervical Spine Injury: An Analysis using Pavlov's Ratio, Spinal Cord Area, and Spinal Canal Area
