Assessment of the Accuracy and Precision of Cystatin C-based GFR Estimates and Cr-based GFR Estimates in Comparison with Cr51-EDTA GFR
- Affiliations
-
- 1Department of Laboratory Medicine, Asan Medical Center and University of Ulsan College of Medicine, Seoul, Korea. wkmin@amc.seoul.kr
- 2Department of Nuclear Medicine, Asan Medical Center and University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 1121657
- DOI: http://doi.org/10.3343/kjlm.2007.27.1.34
Abstract
- BACKGROUND: Cystatin C (cysC) is said to be an ideal marker for glomerular filtration rate (GFR), independent of external factors such as age, nutrition and inflammation. The authors compared the accuracy and precision of cysC-based and creatinine (Cr)-based GFR estimates using Cr51-EDTA GFR method as a reference. METHODS: Serum concentrations of cysC and Cr were measured in adults over 17 yr (n=170) and children below 17 yr (n=79) who had had GFR estimated by Cr51-EDTA method. CysC-based GFR was estimated by the formula of Thierry [CysC-based GFR estimates (mL/min/1.73 m2)=78 x (1/cysC, in mg/L)+4] and Cr-based GFR by the formula of modified Modification of Diet in Renal Disease [MDRD II, Cr-based GFR estimates (mL/min/1.73 m2)=186 x (Scr)(-1.154) x (Age)(-0.203) x 0.742 (for a female patient) x 1.212 (for a black patient). RESULTS: In comparison with Cr51-EDTA GFR, in children below 17 yr, the bias +/- standard deviation (SD) of cysC-based and Cr-based GFR estimates were 7.5 +/- 6.1 and 106.5 +/- 98.2, respectively, in the range of below 90 of Cr51-EDTA GFR (mL/min/1.73 m2), and 33.7 +/- 33.0 and 174.4 +/- 18.8 in the range of over 90. In adults over 17 yr, the respective figures were 13.1 +/- 11.0 and 17.4 +/- 29.8 in below 90, and 21.2 +/- 20.1 and 83.6 +/- 108.8 in over 90 of Cr51-EDTA GFR. CONCLUSIONS: CysC-based GFR estimates show acceptable ranges of biases over the whole age and GFR ranges. CysC-based GFR estimates is considered to be the marker for GFR, which could be used without limitation of age and GFR ranges.
MeSH Terms
Figure
-

Fig. 1. The scatter plot of cystatin C-based GFR estimates (A) and creatinine-based GFR estimates (B) in comparison with Cr51-EDTA GFR.
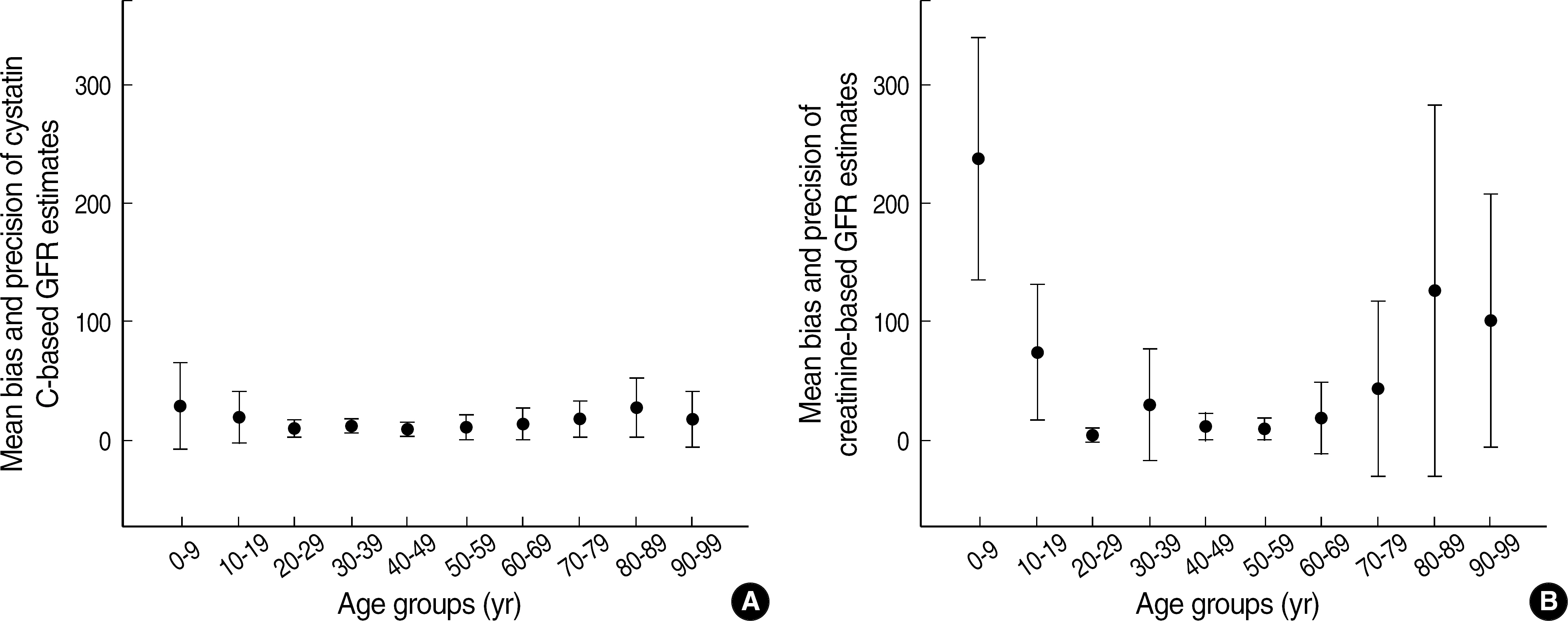
Fig. 2. The mean bias±standard deviation (SD) of Cystatin C-based GFR estimates (A) and Cr-based GFR estimates (B) according to the age groups. Solid circle indicates mean bias in each age group and the length of solid line connecting horizontal solid lines indicates the extent of SD in each group. Cystatin C-based GFR estimates showed the bias less than 30 in the range of 0–99 age groups in contrast to Cr-based GFR estimates showing the bias less than 30 in the range of 20–69 age groups only.
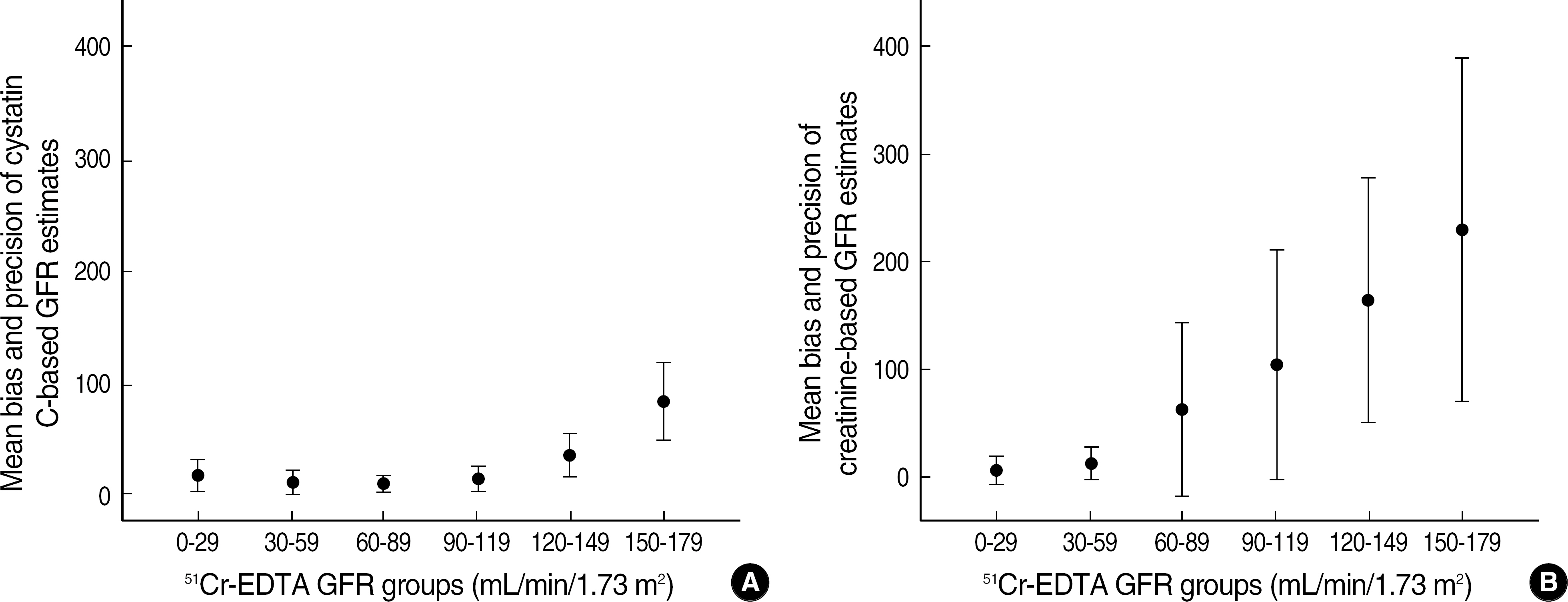
Fig. 3. The mean bias±standard deviation (SD) of Cystatin C-based GFR estimates (A) and Cr-based GFR estimates (B) according to Cr51-EDTA GFR groups. Solid circle indicates mean bias in each Cr51-EDTA GFR group and the length of solid line connecting horizontal solid lines indicates the extent of SD in each group. Cystatin C-based GFR estimates showed the bias less than 30 in the range of 51Cr-EDTA GFR 0–119 (mL/min/1.73 m2) groups in contrast to Cr-based GFR estimates showing the bias less than 30 in the range of 51Cr-EDTA GFR 0–59 (mL/min/1.73 m2) groups only.
Reference
-
References
1. Lamb E, Newman DJ, Price CP. Kidney function tests. Burtis CA, Ashwood ER, Bruns ED, editors. eds.Tietz textbook of clinical chemistry and molecular diagnostics. 4th ed.Philadelphia: Elsevier Saunders;2006. p. 818–26.2. Levey AS, Coresh J, Balk E, Kausz AT, Levin A, Steffes MW, et al. National Kidney Foundation practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Ann Intern Med. 2003; 139:137–47.
Article3. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002; 39(S1):S1–266.4. Le Bricon T, Thervet E, Froissart M, Benlakehal M, Bousquet B, Legendre C, et al. Plasma cystatin C is superior to 24-h creatinine clearance and plasma creatinine for estimation of glomerular filtration rate 3 months after kidney transplantation. Clin Chem. 2000; 46:1206–7.
Article5. Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003; 41:1–12.
Article6. Mussap M, Plebani M. Biochemistry and clinical role of human cystatin C. Crit Rev Clin Lab Sci. 2004; 41:467–550.
Article7. Newman DJ, Thakkar H, Edwards RG, Wilkie M, White T, Grubb AO, et al. Serum cystatin C measured by automated immunoassay: a more sensitive marker of changes in GFR than serum creatinine. Kidney Int. 1995; 47:312–8.
Article8. Cataldi L, Mussap M, Bertelli L, Ruzzante N, Fanos V, Plebani M. Cystatin C in healthy women at term pregnancy and in their infant newborns?: relationship between maternal and neonatal serum levels and reference values. Am J Perinatal. 1999; 16:287–95.
Article9. Fischbach M, Graff V, Terzic J, Bergere V, Oudet M, Hamel G. Impact of age on reference values for serum concentration of cystatin C in children. Pediatr Nephrol. 2002; 17:104–6.
Article10. Norlund L, Fex G, Lanke J, Von Schenck H, Nilsson JE, Leksell H, et al. Reference intervals for the glomerular filtration rate and cell-proliferation markers: serum cystatin C and serum beta 2-microglo-bulin/cystain C-ratio. Scand J Clin Lab Invest. 1997; 57:463–70.11. Finney H, Newman DJ, Price CP. Adult reference ranges serum cystatin C, creatinine and predicted creatinine clearance. Ann Clin Biochem. 2000; 37:49–59.12. Erlandsen EJ, Randers E, Kristensen JH. Reference intervals for serum cystatin C and serum creatinine in adults. Clin Chem Lab Med. 1998; 36:393–7.
Article13. Uhlmann EJ, Hock KG, Issitt C, Sneeringer MR, Cervelli DR, Gorman RT, et al. Reference intervals for plasma cystatin C in healthy volunteers and renal patients, as measured by the Dade Behring BN II System, and correlation with creatinine. Clin Chem. 2001; 47:2031–3.
Article14. Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, Rossert J, et al. Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2005; 67:2089–100.
Article15. Wiesli P, Schwegler B, Spinas GA, Schmid C. Serum cystatin C is sensitive to small changes in thyroid function. Clin Chim Acta. 2003; 338:87–90.
Article16. den Hollander JG, Wulkan RW, Mantel MJ, Berghout A. Is cystatin C a marker of glomerular filtration rate in thyroid dysfunction? Clin Chem. 2003; 49:1558–9.
Article17. Fricker M, Wiesli P, Brandle M, Schwegler B, Schmid C. Impact of thyroid dysfunction on serum cystatin C. Kidney Int. 2003; 63:1944–7.
Article18. Risch L, Herklotz R, Blumberg A, Huber AR. Effects of glucocorticoid immunosuppression on serum cystatin C concentrations in renal transplant patients. Clin Chem. 2001; 47:2055–9.
Article19. Tokyol C, Koken T, Demirbas M, Dilek FH, Yorukoglu K, Mungan U, et al. Expression of cathepsin D in bladder carcinoma: correlation with pathological features and serum cystatin C levels. Tumori. 2006; 92:230–5.
Article20. Saleh Y, Sebzda T, Warwas M, Kopec W, Ziolkowska J, Siewinski M. Expression of cystatin C in clinical human colorectal cancer tissues. J Exp Ther Oncol. 2005; 5:49–53.21. Demirtas S, Akan O, Can M, Elmali E, Akan H. Cystatin C can be affected by nonrenal factors: a preliminary study on leukemia. Clin Biochem. 2006; 39:115–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Relationship between serum cystatin C and glomerular filtration rate in renal transplant patients
- Evaluation of Glomerular Filtration Rate by Prediction Equation in the Elderly
- Comparison of serum cystatin C and creatinine as a marker for early detection of decreasing glomerular filtration rate in renal transplants
- Comparison of various methods of glomerular filtration rate measurements in children
- Evaluation of Serum Cystatin C Concentration as a Marker of Renal Function in Liver Cirrhosis Patients
